Download
1 / 26
280 likes | 676 Views
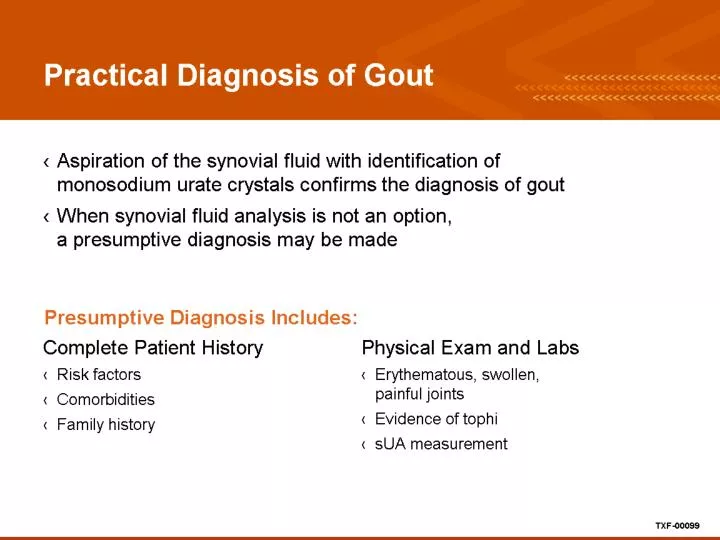
Practical Diagnosis of Gout. Caveat on urate levels. Serum uric acid level may be normal at the time of an acute attack. Normal level does not rule out gout. May be better to recheck the level after 2 weeks. Differential Diagnosis of Gout. Treatment of Gout. Gout Management Approach.

E N D
Caveat on urate levels • Serum uric acid level may be normal at the time of an acute attack. • Normal level does not rule out gout. • May be better to recheck the level after 2 weeks
Resolve the acute flare rapidly • NSAIDs • Corticosteroids • Colchicine Remember that above may all be limited by comorbidities !! Antiinflammatories do not treat the underlying disease.
Evidence for the Use of Concomitant Anti-Inflammatory Prophylaxis
Evidence Supporting ContinuousLowering of Serum Urate to <6 mg/dL
Reduction in Recurrent Gout Flares When sUA Levels Are Maintained at <6 mg/dL
Conclusions Long term approach
Allopurinol • Purine “backbone” xanthine oxidase inhibitor • FDA approved in 1966, most widely used urate-lowering drug for the last four decades. • Basis for the 1988 Nobel Prize in Physiology and Medicine. • Starting dose of 50-100mg daily and slowly titrate; consider prophylaxis against flare. • Some studies suggested that only 21% of patients on 300mg achieved urate level < 6.0.
New and Emerging Gout Meds • febuxostat– oral nonpurine xanthine oxidase inhibitor FDA approved in 2009 for gout and hyperuricemia • pegloticase – PEGylated uricase; not yet FDA approved-- for advanced tophaceous gout, administered intravenously.
Febuxostat • FDA approved doses are 40mg and 80mg. • Published RCT looked at higher doses as well. • Compared to allopurinol, was as good or superior in achieving goal of sUA <6.0. • Significant reduction in gout flares and tophi when sUA goal is maintained.
ULORIC A Allopurinol has a purine backbone. Febuxostat is a non-purine xanthine oxidase inhibitor. Febuxostat
Febuxostat • Primarily excreted by the liver, only 3% by the kidney; no dosage reduction required for renal impairment. • Mild transaminase elevations observed, similar to that of allopurinol. • Contraindicated with use of 6-MP, azathioprine, theophylline • In RCT a higher rate of CV and thromboembolic events noted (0.14 / 100 pt-years > allopurinol), but a causal relationship not identified
Febuxostat • Primarily excreted by the liver, only 3% by the kidney; no dosage reduction required for renal impairment. • Mild transaminase elevations observed, similar to that of allopurinol. • Contraindicated with use of 6-MP, azathioprine, theophylline • In RCT a higher rate of CV and thromboembolic events noted (0.14 / 100 pt-years > allopurinol), but a causal relationship not identified
Febuxostat • In general 40mg (starting dose) not inferior to 300mg allopurinol. 80 mg dose produced higher rate of achieving target sUA level of <6.0 and reduction of flares • 5-year findings (FOCUS) showed sustained effect with maintenance of sUA < 6.0 and nearly complete suppression of flares
References (febuxostat) • Becker, M.A., et al. NEJM.353:2450, December 8, 2005 {“FACT trial”} • Schumacher, H.R., et al. Rheum. 48; (2),188- 194. {“FOCUS” 5-year findings} • Becker, M.A, et al. Arthr & Rheum, 52; (3), 916-923. • Schumacher, H.R., et al. A&R (Arthr Care & Research). 59; (11), 1540-1548.