Download
1 / 52
540 likes | 827 Views
Cardiology Finals Revision. Andrew Degnan PALI Wednesday 12 th September 2012. Why Cardiology?. Why Cardiology?. 2005 Paper 1-Heart failure Paper 2-Unstable angina Resit 1-Aortic stenosis Resit 2-Infective endocarditis and pericarditis 2006 Paper 1-Heart failure

E N D
Cardiology Finals Revision Andrew Degnan PALI Wednesday 12th September 2012
Why Cardiology? • 2005 • Paper 1-Heart failure • Paper 2-Unstable angina • Resit 1-Aortic stenosis • Resit 2-Infective endocarditis and pericarditis • 2006 • Paper 1-Heart failure • Paper 2-Primary prevention • 2007 • Paper 1-Heart failure and pericarditis • Paper 2-None • 2010 • Paper 1-None • Paper 2-Postural hypotension • Resit 1-Aortic stenosis • Resit 2-Infective endocarditis • 2011 • Mock-Heart failure • Paper 1-None • Paper 2-Infective endocarditis and heart failure • Resit 1-Acute MI • Resit 2-Postural hypotension • 2012 • Paper 1-None • Paper 2-Unstable angina and postural hypotension
2012 Mock Paper Unstable Angina
MEQ 1.8 • A 39 year old Asian man was admitted to the medical admissions unit with pains in his chest and neck. He admitted to smoking 20 cigarettes per day and a blood cholesterol had been measured at 7.2mmol/L (reference range 3.5-5.0mmol/L). His average HR on admission was 90 bpm and his blood pressure was 170/100mmHg. An initial diagnosis of unstable angina was made. (a) • What are his risk factors for coronary artery disease? (2 marks)
MEQ 1.8 • A 39 year old Asianman was admitted to the medical admissions unit with pains in his chest and neck. He admitted to smoking 20 cigarettes per day and a blood cholesterol had been measured at 7.2mmol/L (reference range 3.5-5.0mmol/L). His average HR on admission was 90 bpm and his blood pressure was 170/100mmHg. An initial diagnosis of unstable angina was made.
Risk Factors for CVD Unmodifiable Factors Modifiable Risk Factors Smoking Hyperlipidaemia Obesity (diet and exercise) Diabetes Hypertension Stress • Male • Increasing age • Asian decent • Post-menopause • Family History
(b) • You decide to admit him to hospital. What drug therapy could he be started on? List 4 potentially beneficial drugs (2 marks) and give a reason for prescribing each (2 marks).
Immediate Treatment of NSTEMI and UA • Anti-ischaemic therapy (decrease myocardial oxygen demand) • Nitrates (GTNIV), venodilation, decrease venous return • Beta-blockers, decrease sympathetic drive and so decrease O2 demand • Anti-thrombotic therapy (prevent further development of partially occluded thrombus) • Aspirin, prevents platelet aggregation and activation • Clopidogrel, alternative action on platelets. Can be used in combitaion with or in place of aspirin • Heparin, usually LMWH, breaks down any clots
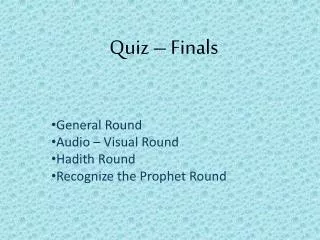
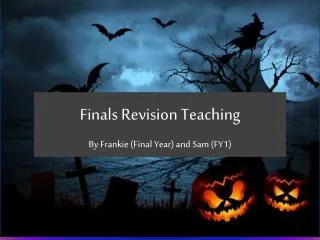
Results of blood tests revealed a Troponin T of 0.35ng/ml (normal=unrecordable), peak CK was 180iu/ml (reference range: 25-200iu/ml) on day 2 (c) • List the 2 cardinal ECG features of an acute full thickness anterior myocardial infarction and outline their electrophysiological cause (4 marks)
The Easy Bit http://en.wikipedia.org/wiki/File:12_Lead_EKG_ST_Elevation_tracing_color_coded.jpg
The Hard Bit Is it enough to answer with “It just does”?
ST Elevation • Changes in the action potentials produced by necrotic tissue • Abnormal firing of action potentials leads to early repolarisation secondary to ischaemia, causing this abnormal wave • Pathological Q Waves • Any initial downward movement of the QRS is a Q wave. • Pathological Q waves are Q waves developing after MI which have a width of ≥ 1 small box and a depth > 25% of the total QRS height • Develop from living tissue behind the infarct which is picked up by the ECG as a downward movement as impulses move away from the anterior leads
Cardiac Enzymes http://en.wikipedia.org/wiki/File:AMI_bloodtests_engl.png
2005 Paper 1 Left Ventricular Failure
MEQ 1.2 • A 78 year old man had a large anterior myocardial infarction three years ago. Initially he made a good recovery, but has had to take a diuretic for ankle swelling since. In the last 2 months he has become short of breath on exertion. You suspect that he has developed left ventricular failure (a) • Give 2 additional symptoms that would support this diagnosis (2 marks)
MEQ 1.2 • A 78 year old man had a large anterior myocardial infarction three years ago. Initially he made a good recovery, but has had to take a diuretic for ankle swelling since. In the last 2 months he has become short of breath on exertion. You suspect that he has developed left ventricular failure (a) • Give 2 additional symptoms that would support this diagnosis (2 marks)
Left Heart Failure Right Heart Failure Peripheral oedema Abdominal discomfort Weight gain Anorexia and nausea • Exertional dyspnoea • Orthopnoea • Paraxysmal nocturnal dyspnoea • Fatigue and weakness • Poor exercise tolerance • Cardiac wheeze • Nocturnal cough with frothy pink sputum • Impaired urine output during the day and nocturia at night • Impaired metal status • Cold peripheries
Left Heart Failure Right Heart Failure Peripheral oedema Abdominal discomfort Weight gain Anorexia and nausea • Exertional dyspnoea • Orthopnoea • Paraxysmal nocturnal dyspnoea • Fatigue and weakness • Poor exercise tolerance • Cardiac wheeze • Nocturnal cough with frothy pink sputum • Impaired urine output during the day and nocturia at night • Impaired mental status • Cold peripheries
Left Heart Failure Right Heart Failure Cachexia Oedema Increased JVP with positive hepatojugular reflex RV heave Hepatomegaly Ankle oedema Sacral oedema Ascities • Cachexia • Cyanosis • Sweating • Tachopnoea • Tachycardia • Pulses alternans • Bilateral basal crackles • Displaced apex beat • Extra heart sounds and murmurs (depends on cause)
(b) • You arrange for a chest X-ray. Give four features that would support the diagnosis of left ventricular failure (4 marks)
Adapted from http://www.e-radiography.net/technique/chest/chest_eval.htm
Adapted from http://www.learningradiology.com/archives2007/COW%20267-Pulmonary%20edema-CHF/caseoftheweek267page.html
Adapted from http://www.radiologysingapore.com/lectures/plain-films-with-diagnosis-6/
(c) • Give 2 neurohormonal mechanisms which may be activated in heart failure (2 marks)
4 Neurohormonal Mechanisms • Sympathetic Nervous System Activity • Fall in CO detected by baroreceptors, sympathetic drive increases, ↑ HR and BP 2. RAAS • Decreasing renal perfusion activates RAAS which ↑ PVR (angiotensin II) and blood volume (aldosterone) which both play a role in ↑ BP 3. ADH • Released in response to low BP and release of angiotensin II. ↑ blood volume and hence BP 4. Natriuretic Peptides • Both ANP and BNP. Both inhibit RAAS and so ↓ blood volume and BP. Beneficial effect, but not released in sufficient enough quantities. BNP=prognostic marker
These all have an effect on…? • Frank Starling Mechanism • Improved venous return improves LV contraction • Preload vs. afterload And this combination leads to • Symptoms of LV HF • Hypertrophy
(d) • If starting this patient on an ACE inhibitor, what precautions would you take? (3 marks)
Side-effects Contra-indications and Cautions Hypersensitivity Bilateral renal artery stenosis Pregnancy Impaired renal function Aortic stenosis Cardiac outflow obstruction Hypovolaemia Haemodialysis • First dose hypotension • Persistent cough • Hyperkalaemia • Renal impairment • Headache • Dizziness • Fatigue • Nausea
Other Precautions • Check baseline BP (first dose hypotension) and Us+Es (hyperkalaemia, renal dysfunction) • Start low, tritrate dose up • Continue to monitor Us+Es • Drug interactions
2011 Paper 2 (also 2005 Resit 1 and 2010 Paper 2) Infective Endocarditis
MEQ 2.6 A 32 year old woman, who is a known alcoholic and abuser of intravenous drugs, presents to A+E complaining of gradual onset malaise, fever, weight loss and night sweats. She is pyrexial (38.5°). She has a pansystolic murmur which is thought to be a new finding and you suspect she has a diagnosis of infective endocarditis (a) • Name 4 additional clinical signsthat may be found on examination in this patient (2 marks)
MEQ 2.6 A 32 year old woman, who is a known alcoholic and abuser of intravenous drugs, presents to A+E complaining of gradual onset malaise, fever, weight loss and night sweats. She is pyrexial (38.5°). She has a pansystolic murmur which is thought to be a new finding and you suspect she has a diagnosis of infective endocarditis (a) • Name 4 additional clinical signs that may be found on examination in this patient (2 marks)
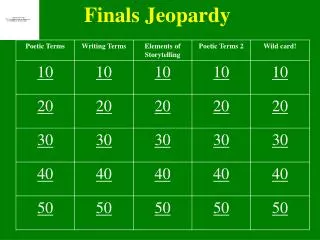
http://medicalpicturesinfo.com/janeway-lesion/ http://en.wikipedia.org/wiki/File:Splinter_hemorrhage.jpg http://en.wikipedia.org/wiki/File:Osler_Nodules_Hand.jpg http://en.wikipedia.org/wiki/File:Acopaquia.jpg
Signs of Infective Endocarditis • Hands • Splinter haemorrhages • Janeway lesions • Osler’s nodes • Clubbing
Signs of Infective Endocarditis • Hands • Splinter haemorrhages • Janeway lesions • Osler’s nodes • Clubbing • Eyes • Roth Spots
Signs of Infective Endocarditis • Hands • Splinter haemorrhages • Janeway lesions • Osler’s nodes • Clubbing • Eyes • Roth Spots • Heart • New murmur • Signs of HF • Others • Abscess • Splenomegaly • Petechia
(b) • Name the 2 most likely organisms likely to be implicated in infective endocarditis (2 marks)
(c) • Your FY2 asks you to dip the urine. What would you expect to find and what is the pathology behind this abnormality? (2 marks) • Blood (microhaematuria) • Pathology • Micro-emboli from vegetation on heart valve • Can block vessels in the glomerulus, causing glomerularnephritis and ARF. • Micro-emboli cause other clinical signs
(d) • Name two investigations that are mandatory to confirm your diagnosis (1 mark)
Blood Cultures • 3 sets • Different times • Different places Major Criteria (x2) • Positive blood culture • Typical organism in 2 separate cultures • Persistently +’ve over time • Echo evidence of valvular involvement • New valvular regurgitation (murmur) • Echo • Trans-oesophageal more sensitive • >2mm for trans-thoracic Minor Criteria (x5) • Risk factors • Fever • Vascular phenomenon • Immunological phenomenon • Positive blood cultures not meeting requirement for major criteria • Echo evidence not meeting requirement for major requirement Dukes Criteria 1 Major + 3 Minor
(e) • Other than IVDU, name 4 risk factors for this condition (2 marks) Environment favourable to Infection Allow Implantations and Growth of Organism Prosthetic heart valve Pre-existing valvular disease Rheumatic Acquired Congenital • IVDU • Dental surgery • Thoracotomy • Catheterisation • Peripheral/central lines • Immunosuppression
On further examination you can also hear the pansystolic murmur. This is loudest at the left sternal edge and you demonstrate the JVP is elevated with giant “v” waves. In addition she also has tender pulsatile hepatomegaly. (f) • What is the most likely cardiac lesion to be responsible for this, given the above history and examination? (1 mark)
Tricuspid Regurgitation On further examination you can also hear the pansystolic murmur. This is loudest at the left sternal edge and you demonstrate the JVP is elevated with giant “v” waves. In addition she also has tender pulsatile hepatomegaly. (f) • What is the most likely cardiac lesion to be responsible for this, given the above history and examination? (1 mark)
Murmurs Systolic Diastolic Quiet Accentuated by manoeuvres Early-mid diastolic Aortic regurge Late diastolic Mitral stenosis Remember DARMS • Loud • Radiate • Ejection Systolic • Aortic Stenosis • Pansystolic • Mitral Regurge