Download
1 / 19
200 likes | 348 Views
Celiac Sprue. December 19, 2005. Definitions. celiac sprue is an immune disorder characterized by inflammation of the proximal small intestine induced by the ingestion of gluten also known as celiac disease and gluten-sensitive enteropathy. History.

E N D
Celiac Sprue December 19, 2005
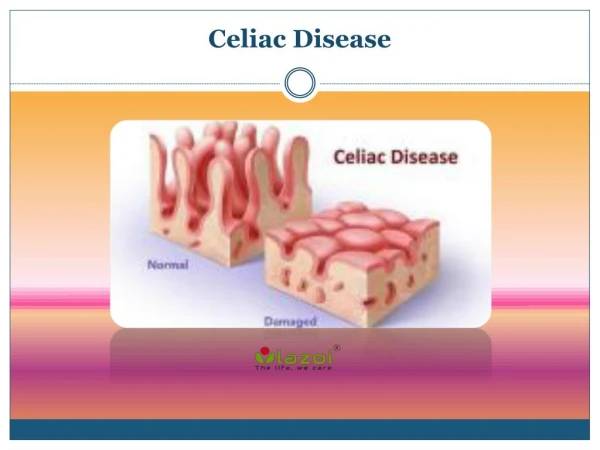
Definitions • celiac sprue is an immune disorder characterized by inflammation of the proximal small intestine induced by the ingestion of gluten • also known as celiac disease and gluten-sensitive enteropathy
History • recognized in the third century (Aretaeus of Cappadocia: chronic diarrhea and “atrophy of the body”) • 1600’s - Dutch term “sprouw” means aphthous disease • Dr. Samuel Gee (UK) in 1888 described the disease and made a link to the diet • Dicke (Dutch pediatrician) linked sprue with wheat during grain shortages in the Netherlands during WWII • 1940’s – water insoluble gluten moiety was causal • 1950’s – small bowel pathology was characterized • 1970’s – first immunoglobulin and autoantibody studies • 1980’s – anti-endomysial antibodies and HLA class II associations (DQ2) • 1990’s – tissue transglutaminase (tTG)
Pathogenesis: Environmental • glutens are water-insoluble grain proteins (prolamins and glutenins) • taxonomy of grains predicts their toxicity in patients Gramineae family Triticum Secale Hordeum Avena Oryza Zea Sorghum Pennisetum genus wheat rye barley oats rice corn sorghum millet grain gliadin secalin hordein avenin oryzenin zein kafirin panicin gluten immunologic cross-reactivity
Pathogenesis: Genetic • concordance • 8-18% in first degree relatives • 70% in monozygotic twins • association with certain HLA DQ haplotypes • 95% of celiac patients are DQ2 • most of the remaining are DQ8 • sprue develops in a minority with DQ2 • 25-30% of Europeans are DQ2 • non-HLA linked gene(s) likely determinant
Classification • classic (typical) celiac sprue • fully expressed form of celiac sprue • symptoms and signs of malabsorption (after breast milk weaning) • atypical celiac sprue • gluten-induced small bowel inflammation • atypical symptoms (anemia, short stature, etc.) • silent celiac sprue • gluten-induced inflammation without symptoms or signs • latent celiac sprue • childhood sprue reverts to normal biopsy and does not recur when gluten is reintroduced (possibly re-develop celiac sprue later in life) • sprue presents later, after earlier documented absence on gluten • potential celiac sprue • abnormal serology but sub-diagnostic biopsy (normal or IELs) • genetic predisposition (DQ2 and/or strong family history) • 50% probability of developing celiac sprue
1:250 Epidemiology celiac iceberg 1:6000 classic atypical silent potential& latent
Childhood Presentation typical failure to thrive diarrhea/steatorrhea anorexia vomiting abdominal distension abdominal pain atypical aphthous ulcers short stature anemia rickets Adult Presentation typical diarrhea/steatorrhea (75-80%) weight loss abdominal bloating/flatulence mild abdominal pain atypical anemia (85%) osteoporosis (15-30%) coagulopathy (10%) aphthous ulcers infertility/menstrual abnormalities neurologic symptoms short stature weakness/myopathy Clinical Presentation
Associated Conditions • dermatitis herpetiformis • rare in childhood; seen in 10% of adult celiac patients • very pruritic • >80% have at least silent or latent sprue, but only 10% of patients have intestinal symptoms • still have 10-40x risk of lymphoma if untreated • type I diabetes mellitus • 3-6% of IDDM patients develop sprue (20x risk) • 5% of sprue patients develop IDDM • IgA deficiency • seen in 10% of sprue patients (complicates diagnosis) • IgA deficient persons have 10x prevalence of sprue • thyroid disease (5% of sprue patients) • autoimmune diseases (Sjögren’s, SLE, PBC) • hyposplenism (~50% of sprue patients) • microscopic colitis
Dietary Guidelines • avoid all foods containing wheat, rye and barley gluten • in Europe, look for gluten-free labels • brand name foods differ from country to country • avoid dairy products (until remission, ~3-6 months) • avoid oats until initial remission, then less than 50-60 grams/day • use only rice, corn, buckwheat, potato, soybean, sorghum or tapioca flour or starches • read all labels and ingredients in processed foods & condiments • watch for gluten in medications, thickeners, emulsifiers and additives • avoid all beers (lagers, ales stouts…) • wine, liqueurs, whiskey, brandy and most ciders are usually OK • consider vitamin, calcium, iron and folate supplementation • remember that medications can be malabsorbed as well • remember that these restrictions are expensive and inconvenient
Response to Diet Restrictions • 70% of patients have symptomatic improvement within 2 weeks • histologic improvement lags unpredictably • may not be evident for 2-3 months • associated with fall in antibody levels in ~3 months • is commonly complete in children • 50% of adults have only partial histologic resolution • failure to respond is most often due to incomplete removal of dietary gluten • with strict adherence… • 5 year survival rate equal to general population • infant and child growth and development normalizes • lower risk of SB lymphoma (back to normal in 5 years)
Complications • refractory sprue • unresponsive sprue (other causes excluded) • may require immunosuppressive therapy or TPN • up to 75% may have cryptic T-cell lymphoma • collagenous sprue • subset of refractory sprue with a poor response and prognosis • ulcerative jejunoileitis (UJI) • ulcers, strictures and severe symptoms (pain, bleeding, obstruction) • high mortality (up to 33%) • higher risk of lymphoma (abnormal clones of T-cells) • malignancy • 3% incidence over 5 year study • SB lymphoma (EATCL) • T-cell origin and often multifocal • accounts for half of malignancies in sprue patients (40x risk) • occurs ~20-40 years after presentation • oropharyngeal and upper GI cancers
Future Directions • bio-engineering gluten-free grains • developing a vaccine or directed therapy against tTG