Download
1 / 42
570 likes | 1.04k Views
Liver cirrhosis. Usama Ahmed Arafa, MD Ass. Professor of Internal Medicine. Definition. Liver cirrhosis is characterized by: 1- Hepatocellular necrosis 2- Hepatic fibrosis 3- Regeneration nodules 4- Loss of architecture. Normal Liver. Cirrhosis. Normal Liver Histology.

E N D
Liver cirrhosis Usama Ahmed Arafa, MD Ass. Professor of Internal Medicine
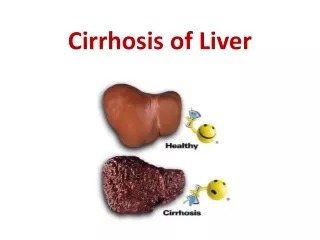
Liver cirrhosis is characterized by: 1- Hepatocellular necrosis 2- Hepatic fibrosis 3- Regeneration nodules 4- Loss of architecture
Normal Liver Histology CV PT
Cirrhosis Fibrosis Regenerating Nodule
Common causes Chronic viral hepatitis: C, B ± D Alcohol Schistosomiasis (fibrosis not true LC) Less Common causes Biliary cirrhosis: - primary - secondary Autoimmune hepatitis Hereditary: - Haemochromatosis - Wilson's disease - Alpha 1 antitrypsin deficiency
Drugs (e.g. methotrexate) • Cystic fibrosis • Non-alcoholic fatty liver disease (NAFLD) • Glycogen storage disease • Veno-occlusive disease • Hepatic venous congestion • Budd-Chiari syndrome • Idiopathic (cryptogenic)
Chronic injury to the liver results in inflammation, necrosis and, eventually, fibrosis. • Fibrosis is initiated by activation of the stellate cells.
In the space of Disse, the normal matrix is replaced by collagen. Subendothelial fibrosis leads to loss of the endothelial fenestrations, and this impairs liver function. • There is accumulating evidence that liver fibrosis is reversible.
Micronodular cirrhosis:Regenerating nodules are usually less than 3 mm in size. This type is often caused by alcoholic or biliary cirrhosis. Macronodular cirrhosis:The nodules are of variable size and normal acini may be seen within the larger nodules. This type is often seen following previous hepatitis. A mixed picture: with small and large nodules is sometimes seen.
A- General manifestations • Wasting • Parotid enlargement • Hyperkinetic circulation • Increased susceptibility to infection
B- Skin manifestations • Spider nevi • Palmar erythema • Leuconychia • Dupuytren’s contractures • Xanthomas • Alternation of body hair distribution
C- Endocrinal manifestations • Gynecomastia • Testicular atrophy • Amenorrhea in females
D- Abdominal manifestations • Hepatomegaly then shrinkage later • Splenomegaly • Prominent abdominal veins • Peptic ulcer disease • Chronic pancreatitis • Steatorrhea
E- Decompensation • Jaundice • Ascitis • Bleeding tendency • Hepatic encephalopathy
Investigations for severity • Liver function. Serum albumin and prothrombin time are the best indicators of liver function. ■ Liver biochemistry. In most cases there is a slight elevation in the serum ALP and serum aminotransferases. ■ Serum electrolytes. A low sodium indicates severe liver disease.
Investigations for the etiology • Viral markers • Serum autoantibodies • Iron indices and ferritin • Copper, ceruloplasmin • Alpha1 antitrypsin (Serum copper and alpha1 antitrypsin should always be measured in young cirrhotics)
Others • Ultrasound examination. • CT scan. • MRI scan. • Endoscopy. • Liver biopsy.
Management is that of complications. • Patients should have 6-monthly ultrasound and serum AFP to detect the development of a hepatocellular carcinoma as early as possible. • There is no treatment that will arrest or reverse the cirrhotic changes although progression may be halted by correcting the underlying cause.
Patients with compensated cirrhosis should lead a normal life. • The only dietary restriction is to reduce salt intake. • Aspirin and NSAIDs should be avoided. • Alcohol should be avoided.
LIVER TRANSPLANTATION • This is an established treatment for anumber of liver diseases. • Shortage of donors is a major problem in all developed countries.
Child's-Pugh classification Score 1 2 3 • Ascites None Mild Moderate/severe • EncephalopathyNone Mild Marked • Bilirubin< 2 mg/dL 2-3 >3 • Albumin> 3.5 (g/dL) 3.5-2.8 < 2.8 • Prothrombintime< 4 seconds 4-6 > 6 (Scores) 1-year survival 5 years 10 years Child's A (< 7) 82 45 25 Child's B (7-9) 62 20 7 Child's C (10+) 42 20 0
Portal hypertension and gastrointestinal haemorrhage • Ascites • Portosystemic encephalopathy • Renal failure (hepatorenal syndrome) • Hepatopulmonary syndrome • Hepatocellular carcinoma • Bacteraemias, infections • Malnutrition