Download
1 / 50
530 likes | 1.28k Views
TRIAGE FOR PCT’S. By Pat Williams, RN, BSN, CEN Clinical Educator City Hospital, Inc. TRIAGE. Objectives Define the concepts and principles of triage List responsibilities of PCT at triage Explain ethical and legal issues at triage Summarize the learnings. TRIAGE.

E N D
TRIAGE FOR PCT’S By Pat Williams, RN, BSN, CEN Clinical Educator City Hospital, Inc.
TRIAGE • Objectives • Define the concepts and principles of triage • List responsibilities of PCT at triage • Explain ethical and legal issues at triage • Summarize the learnings
TRIAGE • TRIAGE-French for “tier” or “sort out” • WWI-sorting of patients to determine treatment priority on battlefields • Military intent was to provide care to the least injured first to go back to battle, then the others were taken care of, the dying were left to die
TRIAGE • Definition: • A system of sorting patients based on the severity of their illness or injury • Each category is predetermined criteria • life-threatening chief complaints • risk for short or long term complications • availability of treatment area and providers
TRIAGE • 3 reasons for triage in the ED • Increased number of cases to be treated • Many patients seeking care in the ED for non-urgent conditions • Efficient use of resources and space
TRIAGE • Primary Objectives • Promptly identify patients requiring immediate, definitive care • Determine the appropriate area for treatment • Facilitate pt. flow through the ED and avoid unnecessary congestion • Provide information and referrals to patients and families
TRIAGE • Primary Objectives-cont. • Allay patient and family anxiety and enhance favorable public perceptions of and experiences with emergency services. • Constant evolution in the type and quality of triage systems • Triage is a necessity in the ED setting • Major component of the EMS & an expected standard of emergency nursing practice.
TRIAGE • ED Triage Systems • Places the RN in the lobby or easily accessible area to entering or waiting patients • Proven to increase patient satisfaction • Screen people for simple information and/or directions
TRIAGE • Triage goals and functions depends on: • Number of patients per day • Type and availability of health-care providers • Availability of specialty treatment area • Environmental, legal, and administrative constraints
TRIAGE • Policies and Procedures • specific to the department • specific to the employee and the expectations
TRIAGE • Comprehensive Triage System • Most advanced triage system • Assessment and prioritization are performed by competent RN’s with proven competency • Use categories to rate patient’s acuity level • Protocols are initiated of specific diagnostic tests, initiation of other treatments, and re-evaluation of the patients.
TRIAGE • TEAMWORK • Triage nurse can not control the number of people walking through the door • Staff is resistant to working triage area, especially when extremely busy • Expectation of the PCT beginning interventions when the patients are taken to the treatment area is UNREALISTIC
TRIAGE • Teamwork, cont. \ • The PCT must return to the triage area as soon as possible, especially during peak and busy hours, as well as when high risk patients/family members are in the lobby • Communication is the KEY when taking a pt. to the room and informing the primary nurse (nurse assigned to that room) of the patients arrival
TRIAGE • Triage Staffing • ED volume • Time of day • Seasonal fluctuations • Patient acuity • Range of triage functions • Staff ability • Rotation of staff every 4,6, or 8 hours.
TRIAGE • Triage is an invaluable, cost-effective asset to any ED. Competent staffing who is assigned to triage could decrease the liability and hospital risks, i.e.: • Making the right choices, assessments, decisions, and treatments • Customer satisfaction • Decrease patient suffering, etc.
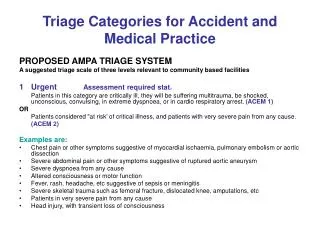
TRIAGE • Decision-making • Done via the interview process and amount of information collected • Emergent: most life-threatening • Urgent: needs immediate assessment, but not life-threatening, etc. • Non-urgent-no fear of loss of life or limb nor any other complications
TRIAGE • Triage Staff • Can “set the tone” for the ED staff, patients, and families as well • Remember to “SMILE” • Introduce yourself • Explain what you are doing • Validate findings • Explain prioritization’s
TRIAGE • Triage Staff, cont. • Explain wait times • Explain rechecking them • Direct to next process • Direct to return to triage if condition changes • Offer comfort measures, i.e. wheelchair, stretcher, blanket, ice bag, splint, sling, etc.
TRIAGE • Triage Staff, cont. • Remember to convey that calm, caring approach during the process to allay the patient and family anxiety and lead to a more comprehensive and successful visit for the patient and family.
TRIAGE • FACTORS FOR QUALITY CARE • Right person • Right place • Right time • Right reasons • Triage nurse: Expected to perform prompt evaluation of all patients entering the ED within 2-5 minutes of their arrival
TRIAGE • Troubleshooting • Confidentiality • Number system for those who wish to not have their name called • Monitor voice and actions • Pull curtain • Remember to use barriers as needed
TRIAGE • Communication • Triage Nurse • Charge Nurse • Registration • Patient Care Tech.’s • EMS • Fast-Track Staff
TRIAGE • Decisions • The TRIAGE NURSE makes the decision who goes to which room first • The time of patient arrival is not the purpose of triage • acuity • symptoms • VS stability • Pain Scale >7
TRIAGE • Other Problems • Lack of decision making skills • Not taking triage position seriously • No advances triage orders, remind RN to write and/or initiate the orders • Not taking patient complaints seriously • List some problems experience, solutions?
TRIAGE • Support • New triage staff need support and reminders • Need support in decision making skills, not criticisms • Need feedback and encouragement • Need patience to improve their efficiency • Identify ways to improve the system • Offer solutions to prevent something from occurring
TRIAGE • Does a nurse to stay in triage at all times? • Yes, a must during peak times and high census times • Discuss legal and ethical reasons for not having a nurse at triage at all times • 7a.m. to 3a.m. RN to be a Triage, foresee, 24-hour RN coverage
TRIAGE • Does the person who performs triage have to be a nurse? • Yes, it is the policy • Non-nursing personnel do not have the authority to make advanced protocol and triage decisions • THE RN IS ULTIMATELY RESPONSIBLE FOR ALL TRIAGE DECISIONS.
TRIAGE • Functions of PCT at Triage • Vital signs on patients • Assist patients to and from registration, to the assigned room, x-ray, or other treatment area • Assist with re-assessing patients in the lobby • Patient advocate to the family/visitors • What others functions can be done at Triage?
TRIAGE • What should we do about patients who leave the waiting room after triage but without being seen? • Monitoring the number of walk-outs • Discuss what happens with chart and information • Discuss the importance of re-assessing patients in the waiting room
TRIAGE • KEEPING EVERYONE INFORMED • Communication is the KEY • Informing patients of delay is of the utmost importance • Can’t predict length of stay or how long it will take • Offer comfort measures • Discuss other reasons for information:
TRIAGE • FACTORS THAT COMPRISE QUALITY CARE AT TRIAGE • Know what works • Doing what works • Do what works well • Know what is right
TRIAGE • Legal Considerations • An emergency evaluation must be performed on any individual with an emergency medical condition or a woman in active labor • If the individual’s condition is unstable, then an attempt to stabilize the individual must be done • Level of transportation to treatment area/s must be appropriate
TRIAGE • Highlights • A sign is posted in the Lobby area that indicates that the hospital participates in Medicare and specifies the rights of the people to examination and treatment. Must be in the common language of the population • Medical screening examination or treatments cannot be delayed to inquire about the patient’s method of payment
TRIAGE • JCAHO Standards • Domestic abuse victims are identified by criteria developed by the hospital • Each patient needs to be reassessed at intervals designated by the institution • Each patient’s physical, psychological, and social status is assessed • Need for discharge planning assessment is determined
TRIAGE • JCAHO • Staff members integrate the information from various assessments of the patient to identify and assign priorities to his/her care needs • A Registered Nurse assesses the patient’s need for nursing care in all settings where nursing care is provided
TRIAGE • Transfers • The hospital provides referral, transfer, or discharge of the patient to another level of care, health professional, or setting based on the patient’s needs and the hospital’s capacity to provide care • The patient must consent or provide a written request to be transferred to another facility in the event the patient is stable for transfer
TRIAGE • Special Considerations • Violence in the Emergency Department • Disruptive Clients • Disruptive Family members/visitors • Potential of Psychiatric patients to become agitated and violent • Beware of the emotionally distraught clients or family members especially when advised to loss of a loved one • Any other situations?
TRIAGE • Communicable Diseases • Chickenpox or Shingles • Remove from waiting area to an isolated area, such as a room, out of the way place in the hallway, etc. • Identify some other communicable diseases?
TRIAGE • Immuno-suppressed Patients • Chemo-therapy patients, AIDS, transplant patients, high dose of steroids • Mask them and remove to an area away from the public and other flu’s, colds, viruses, etc. • Reverse type isolation treatment for these patients
TRIAGE • Poor Hygiene • If medically stable, send to shower and give trousers and gown • Place in an area to provide privacy and to keep the odor contained • Beware there may be other injuries, illnesses, or other medical concerns with these patients
TRIAGE • Pediatric Patients • Remember safety issues with these little ones • Remember the parent may be suffering more than the child • Beware of the child’s activity and bed heights, side rails, playing in the trash cans, etc. • List other concerns with pediatric patients?
TRIAGE • Triage from a Motor Vehicle • Use the buddy system • Use C-spine precautions if indicated • Use good body mechanics • List other ideas for getting a patient out of the vehicles?
TRIAGE • Hazardous Waste • Remember to use safety precautions • Beware of the fact that bio-hazards or contamination to materials is a major concern • Look for MSDS sheets or call the 1-800 number for copies of the MSDS sheets, etc. • Discuss other concerns:
TRIAGE • Psychiatric Patients • Beware of their behavior • Speak softly and slowly in short sentences or phrases • Never turn your back to them • Stay near an exit when interacting with a psychiatric patient • Other Pearls from experiences?
TRIAGE • Obstetric Patients • Place in wheelchair to go to L&D • If presenting part is visible or lots of rectal pressure keep patient in ED for quick evaluation to determine if eminent delivery is about to occur • Never send a patient to L&D alone, an employee must accompanying a woman in labor to the unit
TRIAGE • Case Studies (identify what vitals to do and treatments =/comfort measures to be done) • 46yo male presents with syncope and sweating • 32yo female present with abdominal pain and diarrhea • 14yo male c/o wheezing and short of breath • 8yo female injured right wrist skating • 6mo. Old male with crying and fever