Download
1 / 29
320 likes | 348 Views
Sodium and Potassium Imbalance. An approach for primary care Dr Lori Wik October 5, 2019. Disclosures. I have nothing to disclose. Learning objectives. Sodium and Potassium. Sodium Imbalance: key ideas.

E N D
Sodium and Potassium Imbalance An approach for primary care Dr Lori Wik October 5, 2019
Disclosures I have nothing to disclose
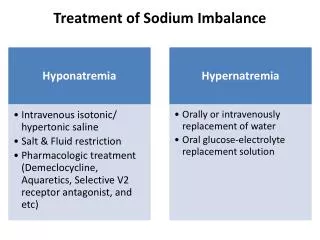
Sodium Imbalance: key ideas • Further laboratory investigations may be appropriate if the clinical assessment and patient history do not reveal the cause of the sodium imbalance • Serum sodium imbalances are more prevalent in older people and hyponatremia is more commonly seen in general practice than hypernatremia • The cause of the sodium imbalance is usually apparent (fluid depletion, medications or volume overload) • Urgent referral to ER is recommended for patients with serum sodium < 120 mmol/L or > 150 mmol/L or if labs are rapidly decreasing or increasing; if neurological symptoms are present or if the patient is systemically unwell
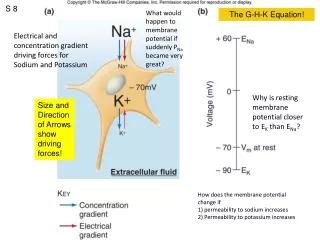
Normal Sodium Hemostasis (surprise! Its all about the water!)
Hyponatremia definition • One of the most common electrolyte imbalances encountered in the office setting • serum sodium < 135 • severe hyponatremia is when serum sodium <120 • The rate of change of sodium is important (rapidly changing sodium is worse than gradual changes) • due to too much water relative to sodium!
Determine the cause: volume status holds the key! • Hypovolemic: dehydration, diarrhea, diuretics, vomiting • Hypervolemic: CHF, cirrhosis, nephrotic syndrome, renal failure • Euvolemic: medications, SIADH, thyroid, adrenal insufficiency
Look for the cause of water loss: normal people do not tend to have high sodium!!
If the cause is not apparent from history • Limited testing can help to sort out the cause: • Urine osmols: high urine osmols (>600) means volume loss/dehydration, low urine osmols (<300) suggests diabetes insipidus • If the patient is stable with a mild or reversible cause of dehydration, it may be safe to treat in the primary care setting with oral rehydration, and close observation.
Potassium imbalance: key concepts • Serum potassium imbalance is more prevalent in older people and people with co-morbidities (renal impairment or congestive heart failure) • Both hypokalemia and hyperkalemia can cause cardiac arrhythmias which may be life threatening • Urgent referral to secondary care is recommended for: • patients with serum potassium ≤ 2.5 mmol/L or ≥ 7 mmol/L • rapidly decreasing or increasing labs • neuromuscular symptoms or ECG changes • if the patient is systemically unwell • The cause of the potassium imbalance is usually clinically apparent, (vomiting, diarrhea, medications or renal impairment) • Further laboratory investigations may be indicated if the clinical assessment and history do not reveal the cause of the potassium imbalance
Lewis J. Disorders of potassium concentration. Merck Manual, 2009. Available from: www.merckmanuals.com https://bpac.org.nz/BT/2011/September/imbalance.aspx
Mechanism of hyperkalemia • Impaired Renal excretion • Renal failure • Hypoaldosteronism (eg: Addison’s) • MRA’s (spironolactone) • Medications that inhibit the RAS (ACEI, ARB, heparin, NSAIDs) • Shift of potassium out of cells (into the bloodstream): • Acidosis (eg: DKA or sepsis) • Digoxin, beta blockers, Septra • Increased circulating potassium: • Cell breakdown (tumor lysis, rhabdomyolysis) • Excessive potassium supplementation, salt substitutes, herbals (milkweed or nettle) • Pseudohyperkalemia
Approach for Dr Wik’s darn CHF medications Extracted from the 2015 ccs heart failure guidelines
Urgent treatment of severe hyperkalemia in hospital/monitored setting
sources • https://bpac.org.nz/BT/2011/September/imbalance.aspx • https://www.onlinecjc.ca/article/S0828-282X(15)00475-4/abstract • Lewis J. Disorders of potassium concentration. Merck Manual, 2009. Available from: www.merckmanuals.com • https://bpac.org.nz/BT/2011/September/imbalance.aspx
Thank you! Any questions???