Download
1 / 85
860 likes | 1.03k Views
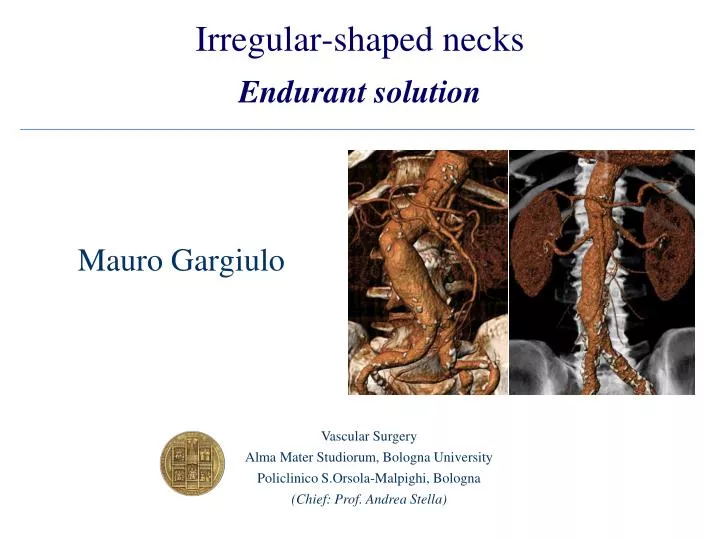
Irregular-shaped necks Endurant solution. Mauro Gargiulo. Vascular Surgery Alma Mater Studiorum, Bologna University Policlinico S.Orsola-Malpighi, Bologna (Chief: Prof. Andrea Stella). How many patients with infrarenal aneurysms are candidates

E N D
Irregular-shaped necksEndurant solution Mauro Gargiulo Vascular Surgery Alma Mater Studiorum, Bologna University Policlinico S.Orsola-Malpighi, Bologna (Chief: Prof. Andrea Stella)
How many patients with infrarenal aneurysms are candidates for endovascular repair? The Northern California Experience Arko FR et al. J Endovasc Ther 2004; 11: 33-40 98 / 220 pts (45%) anatomically unsuitable candidates for EVAR Primary reason for endovascular repair ineligibility by gender
How many patients with infrarenal aneurysms are candidates for endovascular repair? The Northern California Experience Arko FR et al. J Endovasc Ther 2004; 11: 33-40 98 / 220 pts (45%) anatomically unsuitable candidates for EVAR Primary reason for endovascular repair ineligibility by gender
AAA – Neck Characteristics Short neck Aortic angle > 60° Short neck + Aortic angle > 60°
AAA – Neck Characteristics Hostileneck Short neck Aortic angle > 60° Short neck + Aortic angle > 60°
Identifying and grading factors that modify the outcome of endovascular aortic aneurysm repair Chaikof EL et al. JVS 2002 Hostile Neck
AAA – neck lenght ≤ 1 cm Severe Neck 10 mm
Eurostar, J Endovasc Ther 2006;13:640–648 Freedom from proximal endoleak Neck LenghtA >15mm B 11-15mm C <10mm
The correlation of aortic neck lenght to early and late outcomes in endovascular aneurysm repair patients AbuRahma AF et al JVS 2009; 50: 738-48
The correlation of aortic neck lenght to early and late outcomes in endovascular aneurysm repair patients AbuRahma AF et al JVS 2009; 50: 738-48
AAA – Hostile Neck Treatment of choice ? • No treatment • Surgery • EVAR
AAA – Hostile Neck Treatment of choice ? • No treatment • Surgery • EVAR
Endovascular versus Open Repair of Abdominal Aortic Aneurysm The United Kingdom EVAR Trial Investigators NEJM 2010; 362: 1863-71 • Randomized trial • 37 hospitals • Inclusion criteria • - sex: male, female • - age: ≥ 60 years • - AAA diameter: ≥ 5.5 cm • patients anatomically and clinically suitable for either open • surgical repair or endovascular repair
Endovascular versus Open Repair of Abdominal Aortic Aneurysm The United Kingdom EVAR Trial Investigators NEJM 2010; 362: 1863-71 Results • Recruitment: September 1999 – August 2004 • Patients who did not undergo aneurysm repair: 36 • mortality within 6 months: 16.6%
AAA – Hostile Neck Treatment of choice ? • No treatment • Surgery • EVAR
Endovascular repair of Aortic Aneurysm in Patients Physically ineligible for Open Repair NEJM 2010; 362: 1872-80 • EVAR vs BMT in pts unfit to conventional open repair • EVAR 30-days mortality was 7.3% • BMT: overall rate of AAA rupture 12.4/100 person/year • Aneurysm related mortality was lower in the EVAR group (p=0.02) • This advantage did not result in any benefit in terms of total mortality • Conclusion: • EVAR, as compared with no intervention was associated with a significantly lower rate of aneurysm-related mortality in the long term, but with no reduction in total mortality. • Endovascular more expensive
AAA with Severe infrarenal Neck Endovascular Treatment
AAA with Severe infrarenal Neck Endovascular Treatment • Endograft with suprarenal fixation • Primary stenting and standard endograft • “Chimney Technique” • Fenestrated aortic endograft • Large stent graft
AAA with Severe infrarenal Neck Endovascular Treatment • Endograft with suprarenal fixation • Primary stenting and standard endograft • “Chimney Technique” • Fenestrated aortic endograft • Large stent graft
Technology improvements to overcome the challenges in AAA EVAR • Supra-renal fixation devices Endurant
Technology improvements to overcome the challenges in AAA EVAR • Supra-renal fixation devices • High flexibility, conformability and … Endurant
Technology improvements to overcome the challenges in AAA EVAR • Supra-renal fixation devices • High flexibility, conformability and low profile of the delivery system - 14-20F - hydrophilic coating Endurant
Endurant stent-graft system: preliminary report on an innovative treatment for challenging abdominal aortic aneurysm. Verhagen HJM et al. J Cardiovasc Surg 2009; 50: 153-8 • n. Pts 40 (8 Centers) • Mean aneurysm diameter 57,2 mm (46-74) • Neck • mean diameter 24,2 mm (18-30) • mean length 28,9 mm (12-73) • β angle • - 60° - 75° 6 pts (15%) • - < 60° 34 pts (85%)
Endurant stent-graft system: preliminary report on an innovative treatment for challenging abdominal aortic aneurysm. Verhagen HJM et al. J Cardiovasc Surg 2009; 50: 153-8 • Results (30 days) • primary technical success: 90.3% • early type I - III endoleaks 0 • conversion 0 • migrations / thrombosis 0 • mortality 0
Endurant European Trial Courtesy of Verhagen HJM et al. • n. Pts 80 (8 Centers) • Results - 30 days • primary technical success: 91% • early type I endoleaks or III endoleaks 2,6% • - secondary procedure 3.8% • late type I endoleaks or III endoleaks 0 % • migrations / thrombosis 0 % • conversion 0 % • mortality 0 % • Results – 6 months • - no rupture, new type I/III endoleaks, • loss of device integrity, graft infection, • graft thrombosis, stent graft occlusion, • conversion to open surgery, aneurysm expansion, • stent graft migration,loss of stent graft patency
Vascular Surgery – Bologna University • September 2008 – August 2010 • AAA with extreme hostile anatomy • EVAR using Endurant™ stent-graft • Preoperative evaluation: • - CTA and Center Lumen Line Analysis • Prospective data-base
Vascular Surgery – Bologna University Data Base • Demographics (15 variables) • Neck morphology (6 variables) • Morphology of AAA and iliac arteries (7 variables) • Results (short-term, long-term) (8 end points)
Vascular Surgery – Bologna University Data Base • Demographics (15 variables) • Neck morphology (6 variables) • Morphology of AAA and iliac arteries (7 variables) • Results (short-term, long-term) (8 end points)
Vascular Surgery – Bologna University • AAA - Neck anatomy • - diameter • - lengt (renal artery to AAA) • - α angle, β angle • - calcification, thrombosis α β
Vascular Surgery – Bologna University • AAA – Hostile Neck anatomy • - Length (distal renal artery to AAA) ≤ 10 mm • - α angle, β angle ≥ 60° • - Calcification ≥ 50% β α A B C D
Vascular Surgery – Bologna University • AAA – Tortuos Iliac Anatomy • - at least 1 angle > 90° between aortic bifurcation and CFA E
Vascular Surgery – Bologna University The presence of at least one :
Vascular Surgery – Bologna University • Follow up:
Vascular Surgery – Bologna University • Endpoints • - Primary technical success • - Short-term clinical success • Reporting Standards for endovascular aortic aneurysm repair • (Ad Hoc Committee for Standardized Reporting Practices in Vascular Surgery of the SVS/AAVS). • Chaikof E.L. et al. J Vasc Surg 2002;35:1048-60.
Vascular Surgery – Bologna University • Data Analysis • Fisher’s Exact Test • - A,B,C,D vs. Type IA endoleak • Kaplan Meier method • survival • free of complications
Results • Hostile anatomy AAA Endurant EVAR: 38/40 pts. • mean age: 76 ± 7,2 aa • risk factors • - Hypertension 38(100%) • CAD 16 (42.1%) • COPD 21 (55.3%) • Serum creatinine >1,5 mg/dl 7 (18.4%) • PAOD 12 (60%) • ASA III 30 (78.9%) • ASA IV 8 (21.1%) • mean AAA diameter (range): 62 mm (43-94)
Results • AAA - neck • Mean diameter 23 mm (18-30) • - Mean lenght 15 mm (5-32) • Mean angles • α 31° (0-80) • β 54 °(24-92)
Results • AAA – iliac axis • Mean CIA diameter 13 mm (10-23) • Mean EIA diameter 8 mm (6-11) • R iliac axis angle 65°(0-144) • L iliac axis angle 76° (30-133)
Results • AAA – Endograft - Bifurcated 35 (92.1%) - Aorto-uniliac 1 (2.6%) - Tubes 2 (5.3%)
Results • Associated manoeuvres • Iuxtarenal angioplasty 32 cases (84.2%) • Oversizing of the body (mean) 18% (range 8-32; SD ± 7.6) • Proximal aortic cuff extension 1 (2.6%) • Iliac leg stenting 7 (18.4%)
Results • AAA – Distribution of the hostile anatomy features
Clinical Case • AAA diameter 72 mm • Proximal aortic neck • - lenght 10 mm • diameter 21 mm • α angle 90 ° • β angle 90° • Common Iliac arteries diameters • right 13.1 mm • left 12.3 mm
We planned: • Spinal anaesthesia • Right-side common femoral artery approach • Endurant endograft • Main Body: ENBF 28 16 C 170 EE • Left iliac limb ENLW 16 13 C120 EE