Download
1 / 27
270 likes | 294 Views
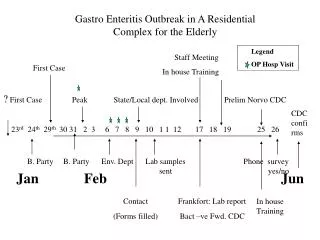
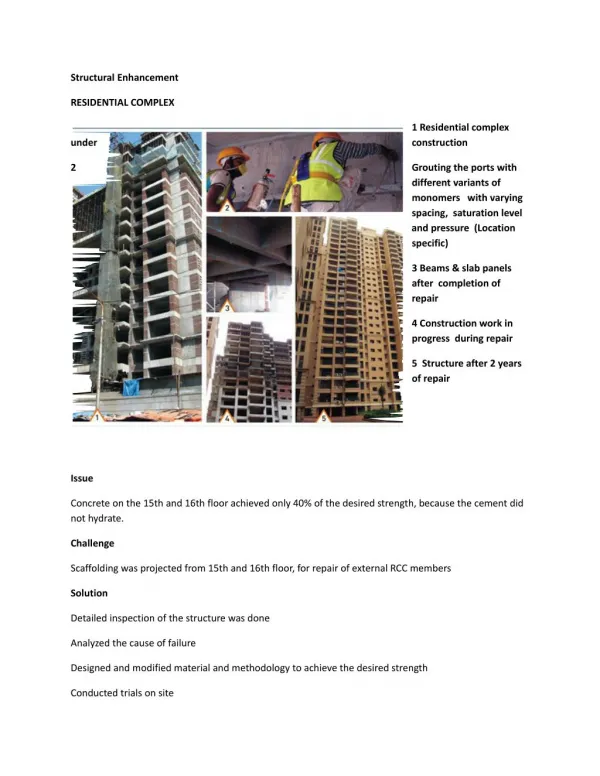
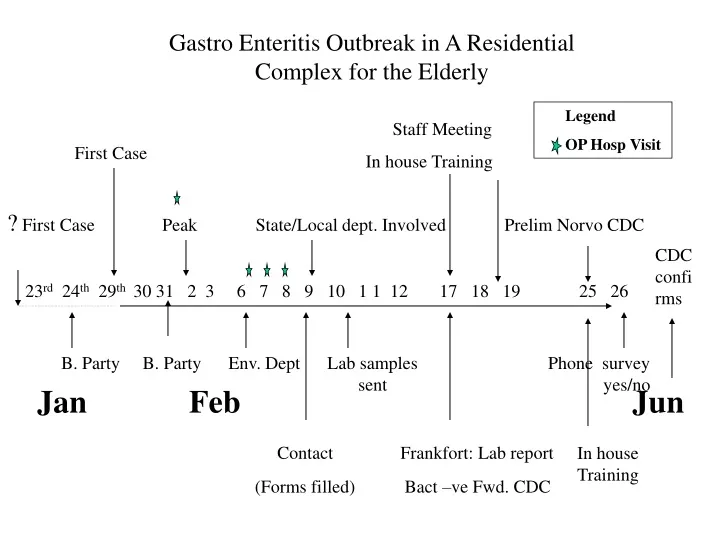
Gastro Enteritis Outbreak in A Residential Complex for the Elderly. Legend OP Hosp Visit. Staff Meeting In house Training. First Case.

E N D
Gastro Enteritis Outbreak in A Residential Complex for the Elderly Legend OP Hosp Visit Staff Meeting In house Training First Case ? First Case Peak State/Local dept. Involved Prelim Norvo CDC CDC confirms 23rd 24th 29th 30 31 2 3 6 7 8 9 10 1 1 12 17 18 19 25 26 B. Party B. Party Env. Dept Lab samples Phone survey sent yes/no JanFeb Jun Contact Frankfort: Lab report (Forms filled) Bact –ve Fwd. CDC In house Training
BACKGROUND Residential Complex for Elderly is 3 tiered Independent Living 61 Occupants Assisted Living 82 Occupants Nursing Home 27 Occupants
Study Objective: • Identify Source and Risk Factors and for the outbreak. • With Emphasis on food-borne disease factors.
ASSISTED LIVING FACILITY RESIDENTS (N = 82) AFFECTED NOT AFFECTED (N= 23) (N= 59) STAFF (N = 35) AFFECTED NOT AFFECTED (N= 13) (N= 22)] STUDY DESIGN: 1:1 Unmatched Case-Control Study. Study Tools : Questionnaire Based Study. Face to face group interview. Telephone survey
Study Setting: • Assisted Living Facility AND some Inputs from • Nursing Home • Independent Living • Main Outcome Measures: • Attack rates at the 3 living facilities for residents • Attack rates for the staff at the assisted living facility • Specific food items related attack rates for the staff
Age of Participants RESIDENTS (N = 82) AFFECTED NOT AFFECTED Mean age 85 Mean age 85 (N= 23) (N= 59) STAFF (N = 35) AFFECTED NOT AFFECTED Mean age 37 Mean age 43 (N= 13) (N= 22)
Results: Figure 1: Common Symptoms
Results: Fig 2 Date of Onset of Illness
Results:Table No. 1 Some Variables Studied for Association in the Assisted Living Facility (Data is only for the Staff) 1. Social Event Gathering No Association. 2. Travel No Association. 3. Child care exposure No Association 4. Drinking water source No Association 5. Spatial clustering No Association
Results Table No 2 (a) Attack Rates Level Total subjects Data Sample Number ill Attack rate Level 1: Independent Living* 61 36 8 25% (8/36) Level 2: Assisted Living** 82 ?82 23 28% (23/82) Level 3: Nursing Home*** 27 27 7 26% (7/27) Assited Living Staff 35 ?35 15 42% (15/35) * Telephone survey to ascertain GI illness in 3-week time frame ** Resident data forms and staff interviews *** Interview with management of Nursing Home
Staff Breakdown Total subjects Data Sample Number ill Attack rate Kitchen 10 10 8 80% (8/10) Other Staff 25 19 5 26% (5/19) Results Table No 2 (b) Attack Rates : Staff
SN Food OR P-Value 95% CI 1. Tomato and Lettuce 0.85 0.83 0.19-3.7 2. Rolls 4.3 0.1 0.8-27.9 3. Soup 0.4 0.3 0.06-2.52 4. Green Beans 0.9 0.6 0.2-4.7 5. Roast Turkey 0.5 0.3 0.09-2.5 6. Cheese 0.6 0.2 0.15-2.9 7. Meat Combo 0.3 0.3 0.03-3.9 Results Table No 3 Risk of GE Associated with Eating of Particular Food amongst staff of a Residential Facility None of these foods were shown to be associated with the illness.
Laboratory Confirmation Lab Specimen sent on: 11th Feb Number & type of specimen: One emesis, one stool Preliminary reports State and CDC: Frankfort Excluded bacteria, forwarded to CDC, CDC reported probable noro virus Final report CDC: June 7th Both samples were tested for norovirus (RT-PCR) When using the Region B primer set, 1 of the 2 samples was positive for norovirus. When using the Region C primer set, 2 out of 2 samples were positive for norovirus. In conclusion, this outbreak of gastroenteritis was associated with multiple strains of norovirus belonging to genogroup II.
Conclusion • The source of outbreak was not likely to be food borne. • The likely spread was person to person. • Clinical, Epidemiological and Preliminary Lab findings are suggestive of Noro virus outbreak. • About half of all GE outbreak in US are Noro Virus Note: Similar outbreaks were being reported throughout US (Virginia, Nevada, Alaska, California) and also in Europe.Europe (Netherlands, Germany, England) reports emergence of a new noro virus variant, a geno group II 4 virus . Lancet 2004;363:682-8.
Lessons Learnt • Functional Aspects • The Hospitals and the HD need to work together. • Establish contact with KY DPH Epidemiology early. • Daily update with Director of the MCHD. • Investigational aspects • 4 Talk to as many people in the facility as possible. • 5 Check tool for appropriateness: large font for elderly. • Notify health providers: They assist in case finding. • Take and specimen containers on initial visit & make specimen collection a top priority
Lessons Learnt • Some useful tools for investigation could be: • i. Large calendar of time frame involved with significant events of the time to help staff and residents be oriented to dates. • ii Group meetings help in standardizing the information people receive and ascertains memories that are agreed upon by the staff. New sources of documented evidence can be unearthed, such as “communication book.”
Shortcomings • Shortcomings of this investigation: • 1. 1) 1/3 of residents have some memory loss • Working through management to obtain individual data has significant limitations. • Delay in obtaining information from staff.