Download
1 / 25
260 likes | 539 Views
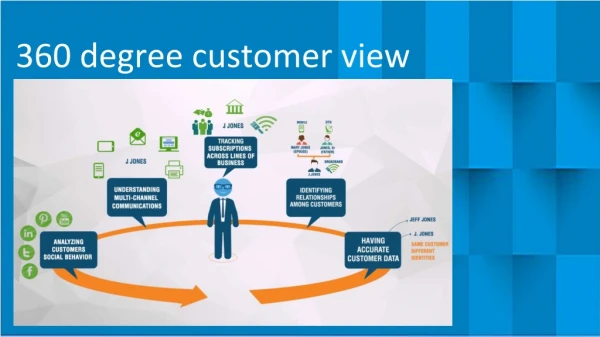
360 Degree Evaluation. Craig McClure, MD May 15, 2003 Educational Outcomes Service Group. Description. Use of rating forms to report frequency of observed behavior Multiple people in contact with resident act as evaluators Often survey type form Ratings summarized by topic

E N D
360 Degree Evaluation Craig McClure, MD May 15, 2003 Educational Outcomes Service Group
Description • Use of rating forms to report frequency of observed behavior • Multiple people in contact with resident act as evaluators • Often survey type form • Ratings summarized by topic • Include goal-setting
Background • Human resources in business • ACGME found no published reports of use in GME
Use for “Soft” Areas • More accurate for formative than summative feedback • Interpersonal & communication • Professional behavior • Limited • Patient care • Systems-based practice
Decision to Utilize • Accepted and used by residents, faculty, staff? • Develop or purchase? • Cost? • Who are the raters? • How will the tool be used?
Decision to Utilize (2) • To whom is the information available? • What core competencies will be evaluated with this tool? • How nurture trust the process remains confidential? • Platform of evaluation
Acceptance • Will all potential evaluators fully participate? • Will raters be fair & honest? • Will residents accept the feedback from non-faculty?
Develop or Purchase • Development permits tailoring • Development time may be considerable • Purchasing gives a ready-made product • Purchasing: computer based
Developing • Expert in educational testing • Programming expertise • Pilot period
Purchase • Items measured appropriate? • Does it perform as claimed? • Inter-rater reliability? • Degree of support and ability to customize
Cost • If purchasing, monetary cost • If developing, personnel support • Data management system • Personnel time to complete forms • Annual development plan
Cost (2) • Addressing EEOC/grievance complaints • Handling disputes over data • Divisive & counterproductive for those resistant
Personnel Evaluation Time • 5 to 10 nurse evaluators per resident to give reproducible results • More for faculty • More for patients
Identify Raters • Patients (how explain process) • Nursing staff • Clerical staff members • Physician faculty members • Non-physician faculty members • Residents
Identify Raters (2) • Medical students • Allied Health Personnel • Self-assessment
Patients as Raters • Literacy • Language • Culture (medical and otherwise) • Personality
Intended Utility • Intervals: monthly, quarterly, yearly • Summative versus formative • To support high stakes decisions?
Access to Information • Resident • Advisor • Program Director
Confidentiality & Trust • Raters require anonymity • Residents require confidentiality • Both need the process to be positive & constructive • Prior history conditions expectations • Education to process aids current participation
Platform of Evaluation • PDA • Paper • Computer
Challenges • Securing appropriate instruments for variety of evaluators • Managing data successfully
Advantages • Electronic database for documentation • Ease of access for raters • Rapid turnaround for feedback • “Gap” analysis (self perception versus image of others)
Disadvantages • Hardware/software costs • Lack of validation in GME • Potential information overload • Selection bias • Discoverability • Potential for invalid feedback
References • Assessment of Communication and Interpersonal Skills Competencies, C.C. Hobgood, et.al. Academic Emergency Medicine 2002;9: 1257-69 • ACGME/ABMS Joint Initiative Toolbox of Assessment Methods, September 2000
References (2) • 360-degree Feedback, K.G. Rodgers,et.al. Academic Emergency Medicine 2002;9:1300-1304 • Letter from ADFM listserv, Goldsmith to Kikano