Download
1 / 37
390 likes | 594 Views
Difficulty Walking – Reasons for and How to Prevent Falls. Michael Sha , MD, FACP Governor, Indiana ACP Chapter Indiana University School of Medicine. 2011 Scientific Meeting Central America ACP Chapter Panama City, Panama. Difficulty Walking. Case:

E N D
Difficulty Walking – Reasons for and How to Prevent Falls Michael Sha, MD, FACP Governor, Indiana ACP Chapter Indiana University School of Medicine 2011 Scientific Meeting Central America ACP Chapter Panama City, Panama
Difficulty Walking • Case: Mr. G is an 82 year old male with chronic obstructive lung disease (COLD, COPD), diabetes mellitus type 2 complicated by neuropathy, s/p “laser treatment” (pan-retinal photocoagulation) for proliferative diabetic retinopathy 2 years ago, and insomnia. He is moving to Panama City to be closer to his children and is coming to the office for the first time. He is accompanied by his son. He kindly waves you away when you ask if he has any problems saying he doesn’t want to bother a busy doctor like yourself.
Difficulty Walking The son becomes visibly frustrated, stands up, and states that all his father does all day, every day is sit in bed and watches soap operas on TV. When you ask him why he lays in bed all day, the patient states that this way he won’t fall. The son adds that the family decided the patient should move in with the son after the patient fell 2 months ago. Since then, the patient has stayed in bed. Notable medications: Statin, Diphenhydramine, Terazosin, aspirin, Lisinopril, Metoprolol, inhaled beta-agonist Vitals: RR 16, T 37 C Orthostatics: recumbent 143/82, HR 55, standing 124/79, HR 60
Difficulty Walking Exam: Frail appearing gentleman who appears pale. The patient is unable to stand without using a “cane” (actually a tree limb that the patient has improvised as a cane). You note he has significant quadricep atrophy. He has a “strange gait” and pain when you internally rotate his left hip.
Difficulty Walking • Difficulty walking = risk for falls • Definition of a “fall” • An unintentional change from a higher body position to a lower position under the influence of gravity • Why does falling matter?
Difficulty Walking • Consequences of falling are magnified in older adults • Injuries like fractures • Impaired independence • Psychological burden • Impaired quality of life • Increased burdens on family members or caregivers • Institutionalization (nursing homes)
Difficulty Walking • One of the more significant consequences of falls is death
Difficulty Walking • How to approach? • In geriatric syndromes, the etiology is almost certainly multifactorial • Evaluate in a systematic fashion • Not necessary to address each problem • The more that you do address, the better the potential outcome
Difficulty Walking - Etiologies • Neurological • Cognitive impairments • Impaired sensory organs • Impaired vision • Impaired hearing • Impaired sensation of the extremities • Vestibular problems • Residual deficits from strokes • Parkinson’s disease or parkinsonism
Difficulty Walking - Etiologies • Cardiovascular • Orthostatic hypotension • Myocardial ischemia • Peripheral arterial disease • Pulmonary • Hypoxia • Obstructive or restrictive lung diseases
Difficulty Walking - Etiologies • Review the medications • Anticholinergics • Antimuscarinic inhibitors – oxybutynin • Antihistamines – loratadine, diphenhydramine • Tricyclic antidepressants – nortriptyline • Sedatives • Muscle relaxers • Antihypertensives – alpha blockers • Psychotropics
Difficulty Walking - Etiologies • Gastrointestinal or Genitourinary • Fecal or urinary incontinence • Benign prostatic hypertrophy • Musculoskeletal • Osteoarthritis • Weakness – particularly proximal muscle weakness
Difficulty Walking - Etiologies • Psychiatric • Fear of falling • Alcohol abuse or another chemical dependency • Metabolic • Vitamin deficiencies (B12, D) • Environment • Night lights • Throw rugs on the floor
Difficulty Walking - Evaluation • Vitals – Orthostatics • Neurological • Assess cerebellar function – finger-to-nose testing, rapid alternating hand movement (dysdiadokinesia) • Assess sensory systems • Romberg - assess for posterior column sense • Strength testing • Proximal muscle weakness – Standing up from a seated position
Difficulty Walking - Evaluation • Musculoskeletal • Internal rotation of the hip – most sensitive maneuver to assess for intra-articular pathology • Assess for leg length discrepancy • Gait • Get-up-and-go test • Observe gait • Tip: watch the patient walk in a hallway
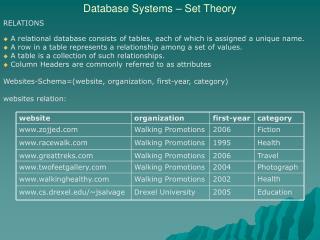
Difficulty Walking - Gait • Normal • Examine the walk • Also need to evaluate for posture, arm swing, speed, number of steps in a turn (http://anatomyresources.hsc.wvu.edu/nm_deficits/Lower_Limb.html)
Difficulty Walking - Gait • Case 1 • Antalgic gait (“a limp”) • Typically an articular pathology affecting one side • Characterized by a shortened stance phase…. after all, it hurts! Charlie Goldberg, MD, University of California, San Deigo
Difficulty Walking - Gait • Case 2 • Parkinsonian gait • Rigid and stooped forward posture • Gait initiation is slow • Hypokinetic • Steps are small and shuffling • Turning is en bloc like a statue • Festinating gait – center of gravity is outside base of support
Difficulty Walking - Gait • Case 3 • Hemiparetic gait • Affected leg is extended with plantar flexed foot • Circumduction of the leg because the leg is too long • Affected arm is adducted, internally rotated with elbow flexion and pronation of the wrist
Difficulty Walking - Interventions • Address “Fear of Falling” • Medications • Physical therapy • Address sensory impairment • Assistive devices • Environment • Medical
Difficulty Walking – Interventions • Fear of falling • Need to address because this frequently results in avoidant behavior • Cognitive behavioral therapy (Zijlstra GA, Journal of the American Geriatrics Society 2009) • Goal – address misconceptions that promote a fear of falling, setting realistic goals for increasing activities, physical therapy to increase strength and balance, and changing the home environment • Intervention – low intensity physical exercises, behavioral contracts, goal setting, lectures, and group discussions
Difficulty Walking - Intervention • Fear of falling • Effective in reducing fear and avoidant behavior • Interestingly, reduced the number of recurrent fallers • 25.5% in intervention, 37.4% in control group (p = 0.02)
Difficulty Walking – Interventions • Medications – Better options! • Insomnia - instead of sedatives, try sleep hygiene or Trazodone • Depression – instead of a tricyclic antidepressant, try an selective serotonin receptor inhibitor (SSRI) • Urinary incontinence – instead of oxybutynin, try a selective muscarinic inhibitor like Solifenacin • Antihistamines – try nasal corticosteroids • Benign prostatic hypertrophy – instead of an alpha blocker, try a selective alpha blocker like Tamsulosin
Difficulty Walking - Intervention • Physical therapy • Focus on gait, strength and balance training • Refer to a therapist or do it yourself • Components • Range of motion • Strength – legs but also arms • Balance • Gait
Difficulty Walking - Interventions • Physical therapy – range of motion and strength • Want to think of planes of motion • Passive range of motion is okay if can’t do active motion • Want to make progress • Think of continuum between range of motion and strength training • Use devices to increase resistance
Difficulty Walking - Interventions • Physical therapy – Balance • Single leg stance • Side leg raise • Hip flexion • Physical therapy – Gait • Tandem walk holding onto a counter or table • http://nihseniorhealth.gov/balanceproblems/toc.html • http://www.eldergym.com/falls-in-elderly.html
Difficulty Walking - Interventions • Address sensory impairments • Appropriate diabetic foot care • Eye exam – glasses to correct vision • Hearing aides • Assistive devices – • Devices to help with walking
Difficulty Walking - Interventions • Assistive devices • Need to be minimally support • Need to be appropriately sized • Need to use appropriately
Difficulty Walking - Interventions • Environment • Remove throw rugs • Elevated toilet seat • Shower chair or bathtub transfer bench • Shower grab bars
Difficulty Walking - Interventions • Medical issues • Address pain and arthritis issues • Could there be a metabolic etiology to the patient’s weakness? • Vitamin D deficiency • Vitamin B12 deficiency • Are the patient’s medical comorbid conditions optimized?
Difficulty Walking - Interventions • Vitamin D (Michael YL, Annals of Internal Medicine 2010) • Evaluated 9 vitamin D supplementation trials • Average oral dose supplement was 800 IU • 17% (95% CI, 11% to 23%) reduced for falls during 6-36 months of follow-up
Difficulty Walking – Prevention • Importance of Exercise (Tanaka H, Journal of Applied Physiology,2003) • Examined VO2max (maximal aerobic capacity) • Correlates well with physical performance, quality of life and independence • Will change and reflect deconditioning and changes in body composition • Select athletes due to training for peak performance
Difficulty Walking – Prevention • Importance of exercise • Found that the rate of VO2max decline was similar in sedentary individuals and master-trained athletes
Difficulty Walking - Prevention • Importance of exercise Disability Sedentary Active Master Athlete
Difficulty Walking - Prevention • Importance of exercise • Physiologic data correlated by epidemiologic data (FeinglassJ, American Journal of Public Health 2009) • Evaluated biennial data from the Health and Retirement Study (HRS) • Assessed almost 6600 respondents who had any difficulty walking and followed them longitudinally for 2 years for any improvement, stability or worsening in ability to walk • Participants who were physically active had OR = 1.4 for improvement in walking ability
Difficulty Walking • Take Home Points • Risk for falling is multifactorial in etiology. Approach systematically…the more you address, the lower the risk for falling • Look at a patient’s gait • Be aware of the “fear of falling” and address it • Physical therapy – you can do it too! • Help with assistive devices • Pick better medicines • Exercise!!
www.acponline.org Questions?