Download
1 / 25
300 likes | 816 Views
Arrhythmias Post Tetralogy of Fallot Surgical Repair. Joseph Atallah, MD CM, SM Division of Pediatric Cardiology Section of Electrophysiology. Outline. Why is there a risk of arrhythmias Arrhythmia classification Recognition Treatment Longterm outcomes Summary. Arrhythmias … Why?.

E N D
Arrhythmias Post Tetralogy of Fallot Surgical Repair Joseph Atallah, MD CM, SM Division of Pediatric Cardiology Section of Electrophysiology
Outline • Why is there a risk of arrhythmias • Arrhythmia classification • Recognition • Treatment • Longterm outcomes • Summary
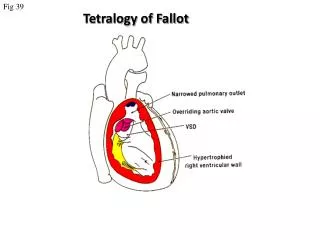
Arrhythmias … Why? • Incidence • Up to 36% of post-op TOF patients will experience some arrhythmic event, mostly insignificant and brief • Majority resolve within 48 hrs post-op • Risk factors • Young age at surgery • Longer bypass and aortic cross-clamp time • Complexity of repair
Arrhythmia Classification • SLOW • FAST .
Arrhythmia Classification • SLOW • Sinus bradycardia • Heart block • FAST • Sinus tachycardia • Atrial tachycardia • Supraventricular tachycardia • Junctional tachycardia • Ventricular tachycardia
Arrhythmia Classification • SLOW • Sinus bradycardia • Intrinsic: sinus node dysfunction (rare) • Extrinsic: medications (sedation …), increased ICP … • Heart block • Results from damage to the AVN, His bundle or bundle branches • FAST • Sinus tachycardia • Common: medications (inotropes, sedation …), hemodynamic stress … • Atrial tachycardia • Rare • Supraventricular tachycardia • ORT or AVNRT or atrial flutter • Junctional tachycardia • Relatively common: multifactorial • Ventricular tachycardia • Rare, more of an issue 10-20-30 years post-op
Heart Block • SLOW • Heart block • Incidence is 1-3% of all pediatric open heart surgeries • Often recognized in the operating room • However, may be acute or gradual in onset in first few days post-op • Highest risk surgeries • LVOTO surgery • VSD Closure • TOF • ccTGA • Definition: more P waves than QRS complexes (more As than Vs)
Heart Block • SLOW • Heart block • 2nd degree (partial) • Not every atrial beat is conducted to the ventricle = ventricular rate is slower than the atrial rate (2:1, 3:1 …) • 3rd degree (complete) • No (zero) atrial beat is conducted to the ventricle • Extreme: HR (VR) = 0 … flat line … bad news … please help! • Most common: ventricular escape rhythm at a certain rate • Inadequate slow vs. acceptable rate • Narrow vs. wide complex QRS
Heart Block QRS QRS QRS ?T P P P P 2 1
Heart Block QRS P P P
Heart Block Narrow QRS Wide QRS
Arrhythmia Recognition • FAST • Supraventricular Tachycardia • Usual rate between 180 and 280 bpm • Sudden onset and termination • Minimal HR variation during SVT • Junctional Tachycardia • Usual rate between 160 and 230 bpm • Gradual onset and termination • HR variation during JET
Junctional Tachycardia • Onset within the first 24 hrs post-op • Due to stress injury around the AV node and the His bundle • Inappropriate accelerated rhythm with the same QRS morphology as sinus rhythm • Often with more Vs then As = VA dissociation • Most common after TOF repair
Junctional Tachycardia QRS V V V V A P A A
Junctional Tachycardia V A V V A V A V A V A
SLOW • Weaning sedation • Warming up • Medications • Atropine • Isoproterenol • Epinephrine • Pacing • Atrial, ventricular or both
FAST • Optimize hemodynamics • Correcting electrolyte and acid-base disturbances • Weaning certain inotropes (e.g. Epi, Dexmetomedine) • Optimizing sedation • Cooling • Anti-arrhythmic drugs • Procainamide • Amiodarone • Esmolol • Overdrive atrial pacing
Long-term Outcomes • Heart Block • At least 60% resolve in the first month post-op • ~90% of those will occur in the first 10 days post-op • Remaining require a permanent pacemaker implantation despite the possibility of late recovery of AV conduction • Supraventricular tachycardia • May resolve • Medical therapy or ablation • Junctional tachycardia • May be very resilient and life threatening • Usually resolves within 2 days but may last 8 days
Summary • Most common arrhythmias post surgical repair of TOF • Heart block • Junctional tachycardia • A simple analytical approach to recognition • Multiple treatment options, ultimately: • Pacing for heart block • AAD for junctional tachycardia • Long-term outcomes: • Heart block: 30-40% will require pacing • ST and JT usually resolve early on