Download
1 / 33
330 likes | 381 Views
Epidemiology, Prevention & Control of Japanese Encephalitis. Introduction. Zoonotic disease Mosquito borne encephalitis Caused by group B arbovirus (Flavivirus) Transmitted by culicine mosquitoes Infecting mainly animals and incidentally man. Japan. Korea. China. India. Philipines.

E N D
Introduction • Zoonotic disease • Mosquito borne encephalitis • Caused by group B arbovirus (Flavivirus) • Transmitted by culicine mosquitoes • Infecting mainly animals and incidentally man
Japan Korea China India Philipines Indonesia Geographic Distribution • 24 Asian and Western Pacific countries • Reduced prevalence in Japan, Korea and China • Estimated 68,000 cases occur each year globally with 20,800 deaths
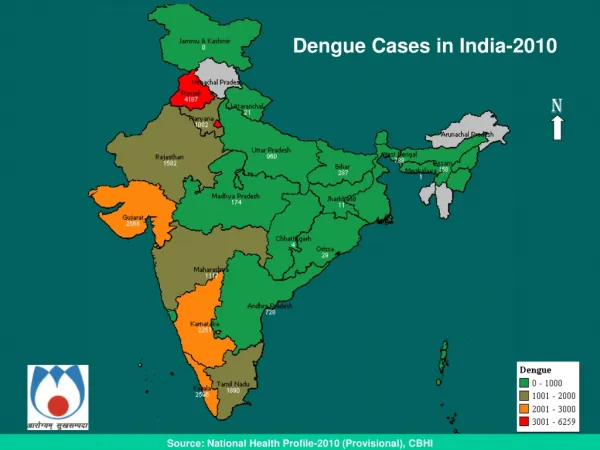
Indian Scenario • Endemic in 21 states, majority cases from UP and Assam • Reported under the umbrella of Acute Encephalitis Syndrome (AES)
Transmission • Rural agricultural location + Flooding irrigation • Enzootic cycle • Mosquitoes: Culex species • Reservoir: Ardeid (wading) birds • Amplifying hosts • Pigs, bats • Possibly reptiles and amphibians • Incidental hosts • Horses, humans
Vectors • C. tritaeniorhyncus, C. vishnui & C. gelidus • C. tritaeniorhyncus is the most important vector in South India • Breeds in irrigated rice fields, shallow ditches and pools • Zoophilic, feeding primarily on vertebrate hosts • After 9-12 days of I.P, transmits the virus to other hosts
JE in man • I.P.5-15 days • Overt disease to inapparent infection ratio is 1:250 • Vast majority of cases among children <15 yrs (85%) • Clinical course • Prodromal stage – fever, headache, malaise for 1-6 days
Clinical Signs: Severe • Acute encephalitis • Headache, high fever, stiff neck, stupor • Severe encephalitis • Paralysis, seizures, convulsions, coma and death • Neuropsychiatric sequelae • 30-50% of survivors • In utero infection possible • Abortion of fetus
Diagnosis and Treatment • Clinical • Laboratory Tests • Tentative diagnosis • Antibody titer • JE-specific IgM in serum or CSF • Definitive diagnosis • Virus isolation: CSF sample, brain • No specific treatment • Supportive care
Acute Encephalitis Syndrome (AES) Case definition: • Acute onset fever not more than 5-7 days duration • Change in mental status with/without • New onset seizures (excluding febrile seizures) • Other early clinical findings-early somnolence/ abnormal behaviour greater than that seen with usual febrile illness
Control Vaccination: • Live attenuated vaccine (SA 14-14-2) • 1 dose of 0.5 ml SC at 1.5 years in endemic districts Vector control: • Aerial or ground fogging with ULV insecticides (malathion, fenithrothion) covering vegetation around the houses, animal shelters, indoor residual spray • Uninfected villages within 2-3 km radius should be brought under spraying
History ….. • Heavy mortality in two species of monkey (Langur & Red faced bonnet ) in 1955 in forests of Shimoga • Mortality in monkeys was followed by acute febrile prostrating illness among villagers and few human deaths
History ……. Autopsy on monkeys Place of reporting of First monkey death in march 1957
Kyasanur forest disease • Found in India • Limited originally to Shimoga district in Karnataka (800 sq km) • Newer foci in 3 more districts - Uttara Kannada, Dakshina Kannada and Chikmangaluru (6000 sq km) • Serosurveys reveal KFD in Kutch & Saurashthra
Problem statement • Outbreak during 1983-1984 is the largest with 2167 cases and 69 deaths. • In 1997, the cases came down to 75 and deaths to 4. • The number of human deaths varied between 4-15% of the cases • Few hundreds of cases and some deaths are reported even today
Agent factors • Febrile disease associated with hemorrhages caused by an arbovirus, flavivirus • KFD virus is a member of group B togaviruses • Belongs to Russian spring summer encephalitis (RSSE) group of viruses
Host factors • Age : Majority between 20 and 40 years • Sex: Males • Occupation: Cultivators who visit forest with cattle or cutting wood • Epidemic correlates with peak human activity in forests i.e between January and June
Natural hosts & reservoirs • Small mammals - rats, squirrels, shrews and bats are the main reservoirs • Neutralizing antibodies have also been found in cattle, buffaloes, goats and porcupines • Monkeys - amplifying hosts
Natural cycle • In enzootic states the infection is maintained in small mammals and also in ticks • When monkeys come in contact with infected ticks , they get infected, amplify and disseminate the infection in “hot spots”of infection • Humans in these hot spots are infected by bite of infected anthrophilic ticks like H.spinigera
Vectors Female tick laying eggs • Hard tick species of the genus Haemophysalis particularly H.spinigera and H.turtura • Ticks act as both as vectors and reservoirs of infection in KFD
Vector bionomics and seasonal transmission • Adult Ticks become active after few monsoon rains in June • Adult population reaches peak during July & August and gradually declines in September • Larval activity builds in post monsoon Oct-Dec • Nymphal activity high from January to May
Vector bionomics and seasonal transmission of KFD • Epidemics coincide with nymphal activity • Nymph most important stage for human transmission (viraemia is significant ) • Adults ticks feed on cattle and viraemia is not significant
Environmental factors • Tropical evergreen, deciduous forests • Clearing of forests for cultivation and other developmental activities leads to change in tick flaura and fauna
Mode Of Transmission • By the bite of infective ticks (nymphal stage) • Humans are dead end in the natural cycle • No evidence of man to man transmission • Transtadial transmission is common in ticks but transovarial transmission is absent except in Ixodides species
Clinical features • Acute phase with sudden onset of fever, headache, severe myalgia with prostation lasting for 2 weeks • GI disturbances and hemorrhagic manifestations in severe cases • Second phase characterized by mild meningoencephalitis after an afebrile period of 7-21 days • Case fatality varies between 4-16%
Diagnosis • Diagnosis by suspicion by clinical signs and symptoms • H/o occupation/travel in forests • Detecting the presence of virus in blood • Serological evidence by haemagglutination and immunofloresence
Treatment Conservative • Antipyretics • Analgesics • Supportive therapy
Control Personal protection • Adequate clothing • Insect repellants such as DMP, DEET provide 90-100% protection against tick bites • Examine themselves for ticks and promptly remove them • Health education
Control of ticks • By aircraft mounted equipment to dispense lindane, cabaryl fenthion at 2.24 kg/ hectare at forest floor • Spraying carried out within 50m around hot spots • Restriction of cattle movement brings reduction in vector population Vaccination • Inactivated chick embryo tissue culture vaccine developed by NIV, Pune • Neutralizing antibodies in 70% of vaccinated persons • Vaccinating at risk population
Bio safety concerns • One of the highest risk category pathogens • Bio safety level 4 • One of the potential bioterrorist weapon