Download
1 / 32
400 likes | 1.28k Views
ACNE. Introduction. One of the commonest skin conditions seen Easily diagnosed May affect mental and social well being Multiple therapeutic options require skill to treat Successful management requires tailormade treatment Affects more than 80% people at some point in their life.

E N D
Introduction • One of the commonest skin conditions seen • Easily diagnosed • May affect mental and social well being • Multiple therapeutic options require skill to treat • Successful management requires tailormade treatment • Affects more than 80% people at some point in their life
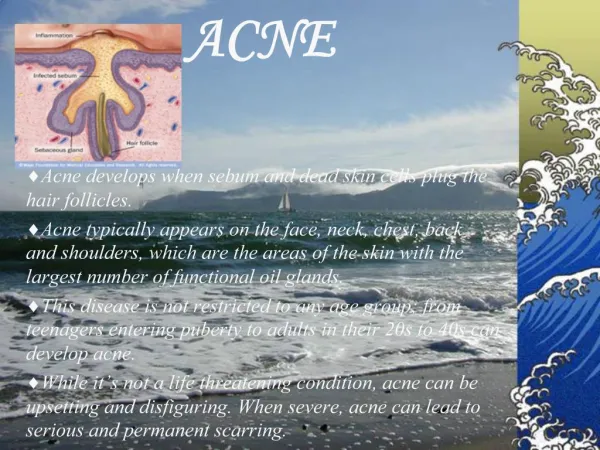
Acne vulgaris Definition: Acne is a chronic inflammatory disease of the pilosebaceous units, characterized by seborrhoea, formation of comedones, erythematous papules, pustules & less frequently by nodules, cysts and scarring.
Epidemiology • Typically occurs around adolescence • Can present in neonate, can persist beyond adolescence in susceptible individuals • Physiological acne considered a normal variant of maturation • Clinical acne persists and progresses beyond the period of adolescence • 30% of teenagers have acne of sufficient severity to require some form of treatment
Pathogenesis of acne • Increased sebum production • Hypercornification of the pilosebaceous duct • Colonisation of the duct with Propionibacterium acnes • Inflammation
Seborrhoea • Increased androgenic sex hormones of gonadal / adrenal origin(especially in women with polycystic ovarian disease) • Abnormal end-organ response to normal level of hormones • Abnormal composition of sebum • Lower levels of linoleic acid → ductalhypercornification
Comedogenesis • Abnormalities in proliferation and differentiation of ductalkeratinocytes • Retention of hyperproliferatingductalkeratinocytes • Increased cohesiveness of ductalkeratinocytes These lead to formation of the microcomedone which is the precursor of all acne lesions
Propionibacterium acnes • Resident anaerobe which colonises the pilosebaceous duct in the presence of seborrhoea • Hydrolyses the triglycerides in sebum to produce free fatty acids • Produces mediators of inflammation • The cell wall of P.acnes is a potent chemoattractant
Inflammation • Cytokines produced by sebum and ductalkeratinocytes • P.acnes & free fatty acids also contibute to the inflammation • Cytokines attract neutrophils and mononuclear cells • In moderate and severe cases there is rupture of the duct and a macrophage giant cell foreign body reaction
Grades of Acne (Pillsburry’s classification) • Grade I: comedones (open or closed), occ. papules • Grade II: papules, comedones, few pustules • Grade III: predominant pustules, nodules, abscesses • Grade IV: mainly cysts, abscesses, scars
Scarring • Consequence of abnormal resolution or wound healing following the inflammation • Ice-pick scars are seen in most patients with grades I and II acne while depressed or hypertrophic scars are seen in nodulocystic acne
Hyperpigmentation • In patients paticularly with type III/IV skin, hyperpigmentedmacules may persist following the resolution of inflammatory acne lesions
Uncommon Variants of Acne • Drug induced acne/ acneiform eruption • Acne excoriee • Acne conglobata • Acne fulminans • Acne mechanica • Occupational acne/chloracne • Pyodermafaciale • Late onset acne/endocrine acne • Cosmetic/pomade acne • Tropical acne • Gram negative folliculitis
Drug induced acne • Papules and pustules , comedones usually absent • Drugs implicated: • Halogens • Androgens • Steroids • INH,Rifampcin • Lithium • Phenytoin • PUVA
Co-factors • Relieving • UV radiation? Aggravating • Premenstrual • UV radiation? • Stress • Sweating • Smoking
Psychosocial aspects • Stress induces acne • Increased anger and anxiety • Social embarrassment • Lack of self confidence • Depression • Dysmorphophobia
Differential diagnosis • Rosacea • Pityrosporumfolliculitis • Pseudo folliculitis • Milia • Plane warts • Tuberous sclerosis • Acne scarring may be mistaken for acne keloidalis, varioliform, atrophy and porphyriacutaneatarda.
Guidelines of treatment • Acne assessment (of severity) • Patient education • Discussion of goals of treatment and patient expectations • Choice of therapy
Guidelines of treatment • Topical antibiotics - erythomycin, clindamycin, tetracycline, clarithromycin, doxycycline • Benzoyl peroxide • Azelaic acid • Topical retinoids - retinoic acid, adapalene, tazarotene
Oral therapy • Antibiotics : Erythromycin Azithromycin (pulse dosing) Tetracycline Doxycycline Minocycline Trimethoprim Dapsone
Side effects of oral antibiotics • Doxycycline - onycholysis, oesophagitis with ulceration, fixed drug eruptions, photosensitivity etc. • Minocycline - benign intracranial hypertension, pappiloedema, blue-black pigmentation and rarely hypersensitivity reactions • Macrolide group - gastritis, diarrhoea • Co-trimoxazole - severe drug reactions • Dapsone - hemolytic anemia, dapsone syndrome etc.
Hormonal therapy • Antiandrogens – cyproterone acetate(50-100 mg/day) • Oral contraceptives - 35 mcgsethinylestradiol plus 2 mgs cyproterone acetate • Levonorgestrel+ethinylestradio (100+20 mcgs) • Other regimens - prednisolone plus oestrogen, spironolactone and antiandrogens • Drosperinone – novel progestin derived from spironolactone • Oral contraceptives containing androgenic progesterones such as norethisterone must be avoided.
Side effects of Hormonal therapy • Weight gain • Menstrual irregularity • Occasional fluid retention • Melasma • Hypertension • Thrombophlebitis • Pulmonary embolism
Isotretinoin 13-cis- retinoic acid (Vitamin A derivative ) • Mechanism of action: • Decreases the size of sebaceous glands • 80% reduction in sebum • Alters the composition of sebum • Reduces comedogenesis • Lowers P.acnes concentration and has anti- inflammatory activity
Isotretinoin • Indicated for : • Nodulocystic/ severe Acne • Pyodermafaciale • Acne recalcitrant to routine treatment • Excessive seborrhoea • Depression / Dysmorphophobia • Acne conglobata / other unusual variants • Scarring
Isotretinoin • Dose: 0.5 – 1 mg/ kg per day is given after meals. Cumulative dose: 120-150 mgs/kg • Side effects • Teratogenicity • Mucocutaneous side effects, dryness • Elevation of serum lipids • Neurological : pseudotumorcerebri, optic • Neuritis, depression, mood swing • Arthritis, myalgia • Acne flares
Physical modalities • Comedo expression • Superficial electrocautery • Aspiration of cystic lesions • Intralesionalsteriods • Cryotherapy • Alpha-hydroxy acids
Newer options • Photodynamic therapy using blue red light • Low fluence pulsed dye laser light • Dermabrasion / CO2laserbrasion (ice-pick scars) • Erbium-YAG laser for atrophic /hypertrophic scars • Punch grafting / punch floats (for depressed scars) • New anti inflammtory agents such as 5-lipooxygenase inhibitors *
Acne treatment plan • Topical therapy for grade I & grade II acne • Oral antibiotics in moderate to severe acne • Combination with topical retinoids improves efficacy and with benzoyl peroxide decreases resistance • Duration 4-6 months • Any treatment started must be continued for atleast 6 weeks before changing • Advise on potential side effects • Systemic isotretinion is indicated in severe nodulocystic acne, acne conglobata and acne recalcitrant to routine therapy Contd..
Acne treatment plan • Hormonal therapy is used for patients with moderate acne who also need contraception, or those who need hormonal therapy to regulate hormonal irregularities • Encourage compliance
Poor response to therapy • Poor compliance • Inadequate instructions • Side effects • Resistance of P. acnes • Inadequate dosage • Folliculitis due to staphylococci, gram negative enterobacteria or malassezia