Download
1 / 27
310 likes | 758 Views
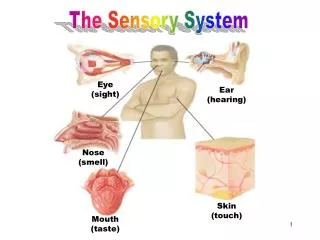
The Sensory System. Examining the sensory system provides information regarding the integrity of the Spinothalamic Tract , posterior columns of the spinal cord and parietal lobes of the brain. Client preparation. Examination gown Sit comfortably on bed or exam table

E N D
Examining the sensory system provides information regarding the integrity of the Spinothalamic Tract, posterior columns of the spinal cord and parietal lobes of the brain.
Client preparation • Examination gown • Sit comfortably on bed or exam table • Explain re position changes • Reassure and provide with clear directions
Equipment • Cotton ball • Objects to feel, quarter or key etc. • Test tubes with hot/cold H2O • Tuning fork, low pitched
Screening Test • Only necessary to evaluate the following • Lateral aspect of upper thighs • Inner aspect of upper arms • Dorsal or palmer surface of hands • Bottom or dorsal surface of feet
Neural Pathways • Sensory impulses travel to the brain via • 2 ascending neural pathways • Spinothalamic tract • Posterior columns Impulses originate in the afferent fibers of the peripheral nerves, are carried through the posterior dorsal root into the spinal cord.
Lateral Spinothalamic Tract • Pain • Temperature • Crude & Light Touch
Posterior Columns • Position • Vibration • Fine touch
Assessment • Scatter stimuli over the distal and proximal parts of all extremities and trunk to cover most of the dermatomes. • Abnormal symptoms may indicate need to test the entire body surface • Pain • Numbness • Tingling
Compare sensations on symmetric parts of the body • If decrease in sensation • Systematic testing • From point of decreased sensation toward sensitive area • Note where sensation changes • Map borders of deficient area, Diagram
Note if the pattern of sensory loss is “distal” • Glove & stocking ( hands & feet) • Dermatones • C3- front of neck • T4 - nipples • T10 – umbilicus • C6 – thumb • L1 inguinal
Dermatones • L4 – Knee • L5 – Anterior ankle & foot Dermatone = bandof skin innervated by the sensory root of a single spinal nerve.
Light Touch Sensation • Use wisp of cotton Ask clients to close both eyes and tell you what they feel and where • Normal Findings • Correctly identifies light touch • In some older clients light touch and pain sensations may be decreased
Abnormal findings • Disorders that can alter perception of sensations • Peripheral neuropathies due to: • Diabetes • Folic acid deficiencies • Alcoholism • Lesions of the ascending spinal cord, brain stem, cranial nerves, and cerebral cortex
Abnormal findings to Touch • Anesthesia = absent • Hypoesthesia = decreased • Hyperesthesia = increased
Pain Sensation • Pin prick • Tongue blade, dull & sharp • Ask to distinguish 2 sec. b/t each stimulus to avoid summation (frequent consecutive stimuli percieved as one strong stimulus)
Abnormalities to pain • Analgesia = absence of pain sensation • Hypalgesia = decreased • Hyperalgesia = increased Apply lightest pressure to obtain response
Temperature • Only tested when pain sensation is abnormal. • Temp. & pain travel in the lateral spinothalamic tract • Test tubes, hot & cold H2O
Vibration • Low pitched tuning fork (128Hz) • Distal interphalangeal joint (finger & big toe) Ask what the patient feels. Ask to tell when the vibration stops and then touch the fork to stop it. If impaired- proceed to more proximal joints or bony prominances.
Posterior Column Tract • Vibration – often first sense to be lost in peripheral neuropathy. • Loss = posterior column disease, lesion of peripheral nerve or root
Position ( Kinesthesia) • Passive movement of extremity • Finger or big toe up and down • Hold by sides b/t thumb and index finger • If position sense is impaired, move proximally to next joint If position sense intact distally , then it is OK proximally.
Tactile Discrimination • Sensory cortex • Eyes closed during testing • Stereognosis= identification of an object by feel • Astereognosis, inability to recognize objects
Number identification= Graphesthesia • Used when stereognosis prevented due to motor impairment for ex. In arthritis • Use blunt end of pen/pencil to draw number • Two-point discrimination • Alternate double with single stimulus • Minimal distance1 from 2 points= less than 5mm on finger pads
Point Localization • Touch pt’s skin • Open eyes and point to where touched • Useful trunk & legs • Extinction • Simultaneously stimulate same area both sides of body • Ask how many points felt and where
charting • If normal • Identifies light touch, dull and sharp sensations to trunk and extremities. • Vibratory sensation, stereognosis, graphesthesia, two-point discrimination intact.
Abnormal results in these tests indicate lesions of the sensory cortex. • These tests not done on children 6 yrs and younger. • 65yrs &older • loss of sensation of vibration at the ankle • Position sense in big toe may be lost • Tactile sensation impaired
Infants and toddlers • Little sensory testing • Hypoesthesia • Responds to pain by crying • General reflex withdrawal of all limbs • 7 – 9mos.can localize stimulus