Download
1 / 13
130 likes | 272 Views
Southern HIV/AIDS Strategy Initiative (“SASI”) : Focusing Federal Attention on the HIV Epidemic in the South. Carolyn McAllaster Clinical Professor of Law Director, Duke AIDS Legal Project I Duke University School of Law

E N D
Southern HIV/AIDS Strategy Initiative (“SASI”):Focusing Federal Attention on the HIV Epidemic in the South Carolyn McAllaster Clinical Professor of Law Director, Duke AIDS Legal Project I Duke University School of Law Project Director, Southern HIV/AIDS Strategy Initiative mcallaster@law.duke.edu
HIV Diagnosis Rate/100,000 population HIV Surveillance Report 2011
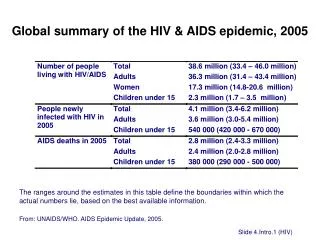
Deaths from HIV Disease, 2010 HIV Death rate: Deaths from HIV per 100,000 population in a given year • 8 of 10 states/district with the highest HIV death rates in 2010 were in the South. • 5 of these states were targeted states (FL, GA, LA, MS, SC). • All of the targeted states were among the 15 states with the highest HIV death rates in the US. Kaiser Family Foundation, State Health Facts (www.statehealthfacts.org)
HIV Case Fatality Rate (2001-2007) HIV Case Fatality Rate: Deaths from HIV per 1000 persons with an HIV diagnosis in a given year • Nine of the 10 states with the highest case fatality rates were in the South; 8 were targeted states (MS, LA, OK, NC, TN, GA, SC, AL, FL). • Mississippi had the highest case fatality rate in the US. *37 states with data from available data; Hanna D, Selik R, Tang T, Gange S. Disparities among states in HIV-related mortality in persons with HIV infection, 37 U.S. STATES, 2001-2007. AIDS. 2011.
Factors Contributing to the Disproportionate HIV Epidemic in the Southern US • Overall poorer health: - 8 of the 10 states with the worst health ratings were in the South in 2012. (http://www.americashealthrankings.org/rankings). • Higher rates of STIs: 8 of 10 states with the highest Chlamydia rates in 2011 were in the South; 6 targeted states.* • Economics: The South has some of the lowest median income figures in the country, as 8 of 10 states with the lowest median incomes from 2010-2011 were located in the South; 5 were targeted Southern states.* • Stigma: Cultural conservatism in the South likely plays a role in stigma for people living with HIV. HIV-related stigma has been found to negatively affect preventive behaviors, care-seeking and adherence, mental health, and quality of care. (http://southernaidsstrategy.org/research/) *Data from Kaiser State Health Facts, statehealthfacts.org
HIV Care Financing Issues • The Ryan White funding inequities for the Southern US, particularly the targeted states, detected in the early 2000s have narrowed, however an estimated gap between the targeted states and the US average in overall Ryan White funding per person living with HIV was $180 in 2011. • The South provided Medicaid coverage for a lower proportion of individuals with HIV in the region when compared to the national average in 2010. Data from Kaiser State Health Facts, statehealthfacts.org
Almost 4 in 10 People with HIV are in States that currently do not Plan to Expand Medicaid ME VT WA NH MT ND MN OR MA NY WI SD ID MI RI CT WY PA NJ IA NE OH DE IN IL NV MD CO UT WV VA CA DC KS MO KY NC TN AZ SC OK AR1 NM GA AL MS AK LA TX FL HI Moving Forward at this Time (25 States including DC) – 55% PLWH Debate Ongoing (4 States) – 8% PLWH Not Moving Forward at this Time (22 States) – 38% PLWH NOTE: As of September 3, 2013 SOURCES: KCMU analysis of recent news reports, executive activity and legislative activity in states. KFF analysis of data from the CDC Atlas.
Loss in Federal $ to non-expansion targeted states The Cost and Coverage Implications of the ACA Medicaid Expansion: National and State-by-State Analysis by Holahan, Buettgens, Carrol, Dorn of The Urban Institute for the Kaiser Commission on Medicaid and the Uninsured, November 2012
Ryan White Going Forward There is a continued need for Ryan White to Address • Gaps in Coverage in non-expansion states: • No Medicaid or subsidies on the insurance marketplace for those with incomes < 100%. • Gaps will exist even for those >100% FPL Need for a mechanism to provide care to PLWHA who are uninsured or uninsured. • Traditional ADAP • Part C Clinics • ADAP wrap-around
Ryan White Going Forward There is a continued need for Ryan White to also address: 2. Gaps in Essential Services • Supportive services essential to linkage to and retention in care • Transportation • Case Management • Part C Clinics • HIV Counseling & Testing • Dental for low-income PLWHA
Questions Going Forward • Full implications of the ACA for PLWHA are unclear. • States can and will continue to expand Medicaid after this year • In those states that do not expand Medicaid, there will be a continued need for Ryan White. • We must engage in an effort to ensure that resources are equitably distributed to reflect the current path of the epidemic and to address the unmet care and treatment needs of low-income persons living with HIV (which post ACA reforms will increasingly and disproportionately be uninsured and underinsured people living with HIV in the southeast U.S.)