Download
1 / 119
1.19k likes | 1.31k Views
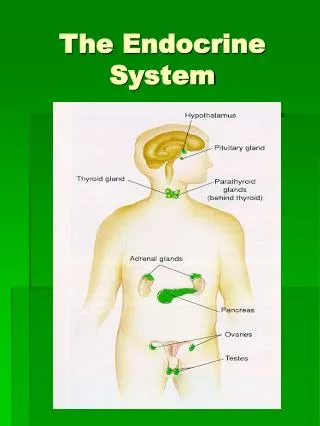
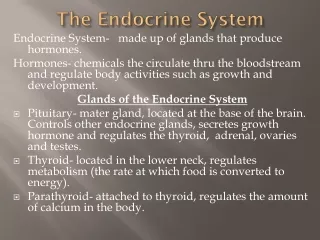
The Endocrine System. Hypothalamus-pituitary axis. The hypothalamic – Pituitary---end organs pathways Corticotrophin-releasing hormone. (CRH) causes a release of ACTH—Adrenal cortex—Mineralocorticoids, androgens.

E N D
Hypothalamus-pituitary axis The hypothalamic – Pituitary---end organs pathways • Corticotrophin-releasing hormone. (CRH) causes a release of ACTH—Adrenal cortex—Mineralocorticoids, androgens.
Gonadotrophins-releasing hormone. (GnRH). Causes a release of LH and FSH—estrogens, progesterone, Testesterone. • Thyrotrophin-releasing hormone. (TRH) releases TSH– thyroid—T3. • Somatostatin (GHIH). Inhibits the releaseof growth hormone.
Somatorelin(GHRH). Release the growth hormone (GH, somatotropin)– IGF, somatomedines. • Dopamine– prolactin---breast.
The pituitary Gland • Consists of anterior and posterior lobes. Anterior pituitary hormones • They are regulated either by releasing or inhibiting factors or hormones.
All are given either IM, IV or intranasally. • They are not given orally (destruction by proteolytic enzymes). 1. Growth hormone (GH). 2. Prolactin.
3. Gonadotrophins (LH and FSH). 4.Adrenocorticotrophic hormone (ACTH). 5.Thyroid stimulating hormone (TSH).
A. Growth hormone (somatotropin) • It is a polypeptide with large MW. • Released in response to GHRH by the
hypothalamus. Hypothalamus secret a growth – hormone releasing factor (GHRF) and a growth- hormone release inhibiting hormone—somatostatin).
Secretion is high in the new born, decreasing at 4 years and maintained until after puberty, when there is a further decline. • Released in pulsatile manner, highest during sleep.
Stimulated by: Hypoglycemia, Fasting and stress. • Inhibited by: insulin-like growth factor I and II (IGF-I, II), glucose, protein and corticosteroids. • GH is produced by recombinant DNA technology.
Effects of GH 1.Stimulation of normal growth and development. 2. Stimulate the production from the liver of several polypeptide mediators, IGFs (somatomedines) responsible for most anabolic actions.
3. Promote protein synthesis, and the uptake of amino acids into cells ( skeletal muscles and cartilage at the epiphyses of long bones), thus influencing bone growth.
Deficiency of GH causes retardation of growth in children- DWARFISM (due to lack of GHRF or IGF generation or action)
GH is produced synthetically by recombinant DNA technology. In short stature, a linear growth can be achieved by given SOMATOTROPINS/C or IM, divide in 6-7 doses per week.
SOMATRIM equal to GH, induces the release from the liver of IGF1(responsible for GH-like effects). • Both have a Half-life 25 min • Cleared by the liver
It should not be given if the epiphysis is closed or suspected intracranial tumour or in acromegaly.
GH over secretion produces a.Gigantism in children. b. Acromgegaly in adults.
Somatostatin • ( Growth hormone-inhibiting hormone) • Inhibits the release of GH, TSH, insulin, glucagon and gastrin.
OCTREOTIDE Is a synthetic analogue of somatostatin. Long acting (T1/2 80 min), depot preparation. Used in acromegaly and pituitary adenomas, tumours secreting vasoactive intestinal peptide, carcinoid tumours and esophageal varices.
Given S/C with peak action in 2h last 8h. may cause: • Pain at the site of injection • GIT upset • Gallstones ( 20-30%) • Hyperglycemia • Hepatitis
B. Prolactin • Is a peptide hormone similar to GH • Secreted by the anterior pituitary (lactotroph or mammotroph cells which are increased in pregnancy due estrogen).
Secretion is inhibited by dopamine. • Stimulated by suckling, TRH, oxytocin and estrogens
Actions • Mammatrophic - for normal development and maturation of the mammary gland. • Lactogenic: during pregnancy
prolactin secretion is high and the level rise steadily towards term. It play a part in milk production.
3.Behavioral: prolactin rises instress, sleep, decreases sexual drive and orgasm.
Hyperprolactinaemia may lead to: Impotence, Hypogonadism, Gynaecomastia, Galactrorrhoea, Amenorrhea.
Treated by BROMOCRIPTINE and CABERGOLINE Prolactin itself is not used clinically.
Bromocriptine • Is a dopamine receptor agonist. • It acts like prolactin inhibitory factor and stimulates inhibitory dopamine receptors, thusinhibiting prolactin secretion.
In acromegaly it suppresses GH release. • Given Orally. • 90% absorbed via the small intestine.
Metabolised in the liver. • Excreted via bile. • T1/2 – 66 hours.
Uses 1. Puerperal lactation can be suppressed. 2.5mg twice/d for 2 weeks. If breast tenderness 2.5mg for 1 week.
2. Hyperprolactinaemia 13% of cases of secondary amenorrhea It may present as infertility, hypogonadism, Galactrorrhoea occurs in 30% of patients.
In men-causes impotence and decrease in volume of semen. • 2.5-7.5mg twice daily for up to 6 months.
3. In the treatment of acromegaly. 4. Parkinson’s disease.
Adverse effects • Constipation, nausea and vomiting, peptic ulcers. • Postural hypotension , dizziness, cardiac arrythmias. • Headache.
4. Nasal congestion, dry mouth vascular spasm, cramps in the legs, pains in extremities, visual hallucination, Cardiac arrhythmias, alcohol intolerance. 5. Psychiatric problems (confusion, hallucination).
C. Gonadotrophins • Gonadotrophin-releasing hormone (GRH)-gonadorelin
Is essential for the release of FSH and LH. • Used to stimulate gonadal hormones production in hypogonadism. • Given IV and S/C • T1/2: 4 min • May cause : allergy, dermatitis and headache.
Synthetic analogs: LEUPROLIDE GOSERELIN HISTRELIN Nafarelin Buserelin Given S/C, Nasal spray, IM T1/2: 3h
They act as inhibitors of GnRH. Used in prostatic cancer, endometriosis and precocious puberty. May cause hot flushes, sweating, decrease libido, depression, osteoparosis and ovarian cysts.
1.Follicle-stimulating hormone (FSH). • Is a glycoprotein. • Secreted in the first part of menstrual cycle from the anterior pituitary.
Stimulate the development of follicle (ovarian). • Stimulate granulosa cell. Increase oestrogen production.
In males stimulate spermatogenesis. Is controlled by Luteinising hormone releasing hormone. (LHRH).
2. Luteinising hormone (LH). • Is a glycoprotein. • Secreted in the second part of menstrual cycle. • Induces ovulation.
Maintains a corpus luteum (progesterone secretion). • In males it stimulate androgen synthesis, and testosterone secretion (play a role in secondary sexual characteristics).
3. Human chorionic gonadotrophin (HCG). • It is derived from the urine of pregnant women which has an actions similar to LH.
MENOTROPINS ( human menopausal gonadotropins, hMG)- obtained from the urine of menopausal women, contains FSH and LH.
Chorionic gonadotropins (hCG), placental hormone, LH agonist, excreted in urine.
UROFOLLITROPIN: FSH devoid of LH, obtained from menopausal women.