Download
1 / 50
510 likes | 615 Views
Osteoarthritis. Definition. Also known as degenerative joint disease or “wear and tear arthritis”. Progressive loss of cartilage with remodeling of subchondral bone and progressive deformity of the joint (s). Cartilage destruction may be a result of a variety of etiologies.

E N D
Definition • Also known as degenerative joint disease or “wear and tear arthritis”. • Progressive loss of cartilage with remodeling of subchondral bone and progressive deformity of the joint (s). • Cartilage destruction may be a result of a variety of etiologies
Prevalence and epidemiology • It’s the commonest form of arthritis • About 60-90% of people over age 65 • Under 45 yrs it is equally common in men and women • Over 55 yrs its more common in women • Nodal OA involving DIP and PIP joints is more common in women and their first degree female relatives
Premature OA associated with gene mutations that encode collagen types 2, 9, 10 • OA of knee is more common in women • Commonest cause of long-term disability • Large economic impact as a result of medical costs
It is not an inevitable part of aging, some people are more susceptible than others • A combination of different factors are involved. • Both mechanical and biologic destructive processes play a role in OA.
Risk factors • Metabolic (hemachromatosis) • Inflammatory (RA, infection) • age • gender • genetic factors • trauma • weight
Primary Idopathic Localized or generalized Local: knee, hip, spine, hands Generalized: large joints and spine Small peripheral joints and spine Mixed and spine Secondary Post-traumataic Congenital or developmental Localized or generalized Calcium deposition disease Classification
Inflammatory OA • OA is generally a non-inflammtory arthritis. • Increasing evidence for inflammatory type: caused by cytokines, metalloproteinase release. • This erosive inflammatory type may have flares but later acts like typical OA. • Primarily in women • May be suspected from evidence of active synovitis, chondrocalcinosis on x-rays, morning stiffness greater than 30 mins, history of swelling and night pain.
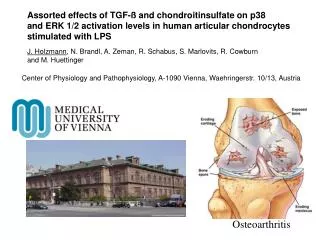
Overview of the process • Articular cartilage gets disrupted • Damage progresses deeper to subchondral bone
Fragments of cartilage released into joint • Matrix degenerates • Eventually there is complete loss of cartilage • Bone is exposed
left: Normal x-ray • Right: worn away cartilage reflected by decreased joint space
The process – at a cellular level • Cartilage matrix has increased water content and decreased proteoglycan • With aging cartilage dries up. • Increased activity of proteinases compared to inhibitors of proteinases. • The cartilage with less water is less resistant to wear and tear. • Cycle of destruction starts • Compensatory bone overgrowth occurs - subchondral bone increases in density
Left: View of normal elbow cartilage through an arthroscope - white, glistening, smooth Right: severe elbow osteoarthritis - cartilage is lost and the bone underneath is exposed
The process cont’d • Bony proliferations at joint margins form, osteophytes • Thought to be new bone formation in response to degenerating cartilage • They cause joint motion restriction
What to look for in an x-ray • Radiographic changes visible relatively late in the disease • Subchondral sclerosis • Joint space narrowing esp where there is stress • Subchondral cysts • Osteophytes • Bone mineralization should be normal
Joint space narrowing where there is more stress • Subchondral bone has thickened • bony overgrowth
significant joint space narrowing as well as proliferative bone formation around the femoral neck (arrows)
Left: normal hip Right: There is some joint space medially but the superior portion is completely destroyed. Supralateral aspects affected most because the weight is transfered through the roof of the acetabulum. Note the sclerosis and oseophyte formation (arrow).
painful bone on bone contact at the CMC joint and the large bone spurs -- osteophytes.
X-ray shows lateral osteophytes, varus deformity, narrow joint space in a 70 yr old female with OA
Clinical features and diagnosis • Pain Sources • Joint effusion and stretching of the joint capsule • Torn menisci • Inflammation of periarticular bursae • Periarticular muscle spasm • Psychological factors • Deep, aching localized to the joint • Slow in onset • Worsened with activity in initial stages • Occurs at rest with advanced disease
May be referred eg hip pain referred to the thigh, groin, knee. • Pain may be aggravated with weather changes
Exam • Joint line tenderness • Bony enlargement of joint • +/- effusion • Crepitus • Decreased range of motion
Joint exam • Joint line pain can indicate tear of the lining of the capsule or the meniscus.
Joint exam • In the evaluation of joint line pain, perform a varus or valgus stress test. • Apply stress across the joint, place fingers directly over the joint line to assess for pain, a clunk may indicate a meniscal tear, or crepitus may indicate cartilage damage.
Have the patient to lie supine on the exam table with leg muscles relaxed • Press the patella downward and quickly release it. • the patella visibly rebounds. • This mean a large knee effusion • Called ballotable patella
Have the patient lie supine with leg muscles relaxed • Compress the suprapatellar pouch with your thumb, palm, and index finger. • "Milk" downward and laterally so that any excess fluid collects on the medial side. • Tap gently over the collected fluid and observe the effect on the lateral side • A fullness on the lateral side indicates the presence small knee effusion
Involved joints • DIP • 1stcarpometacarpal • cervical/lumbar facet joints • 1stmetatarsophalangeal • Hips • Knees • Uncommon • Wrist, elbows, shoulders, ankles
1st metatarso-phalangeal most commonly affected in OA of the foot.
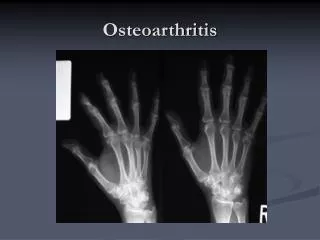
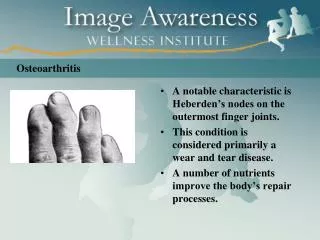
Typical findings • Heberden’s nodes • Bouchard’s nodes
Treatment • Non-pharmacological • No proven medication-based disease modifying intervention exists. • Analgesics (acetominophen/ paracetamol) • NSAIDS Help pain symptoms but controversial for long term use in non-inflammatory OA because of risks vs benefits • Narcotics • Intra-articular steroids • Chondroprotective agents • Anti-depressants
Non-pharmacological rx • Reasonable evidence for efficacy • Exercise – prevent disuse atrophy of muscles • Physical therapy: Hydrotherapy/heat/cold, paraffin baths • Weight loss • Education • Wedges shoe insoles/braces • Refer to physiatrist for management plan.
Analgesics • Paracetamol at doses of up to 4g per day
Opioid analgesics • Generally should be avoided for long term use • For short term rx they may be effective. • In older pts use caution because of side effects such as confusion, constipation, sedation. • Can use tramadol with pcm, in addition to NSAID/COX-2 inhibitor
A controlled study showed codeine and pcm combination to be equivalent to tramadol and pcm • Consider opiates if pt is not a candidate for surgery, or is at high risk for side effects from NSAIDS
NSAIDS • Useful in non-inflammatory OA when pain is moderate to severe • Topical preparations available • PGE2 may contribute to local inflammation and so there is a role for NSAIDS in inflammatory OA
Selective COX-2 inhibitors • They have 200-300 times selectivity for COX-2 over COX-1. • Less gastroduodenal toxicity • Avoid in pts with atherosclerotic CAD - use traditional NSAIDS with a PPI/sucralfate/misoprostol
Side effects • Rash/hypersensitivity • GI bleeding • CNS dysfunction in elderly • Impairment of renal/hepatic/platelet function. How can NSAIDS lead to renal dysfunction? • By interfering with vasodilator renal PG and causing renal ischemia.
Intra-articular corticosteroids • May be used if NSAIDS are contraindicated, persistent pain despite use of other medications. • (not > 2 injections per year per joint) • saline vs. steroid injection? • A study comparing the two in knee OA showed no effect on joint space narrowing or significant difference in pain at the end of the study, but over a 2 yr period saline injections has less pain relief.
Intra-articular hyaluronans • Evidence shows they have a small advantage in terms of pain control, compared to intra-articular placebos or NSAIDS. • No evidence for improvement in function • Two studies comparing intra-articular steroids to hyaluronans have come to opposite conclusions-more trials are needed.
Surgical: arthroscopy • arthroscopy is not recommended for nonspecific "cleaning of the knee“. • Used to fix specific structural damage on imaging (repairing meniscal tears, removing fragments of torn menisci that are producing symptoms).
Joint replacement • If all other rx ineffective, and pain is severe • Loss of joint function • Joints last 8-15 years without complications