Download
1 / 51
520 likes | 766 Views
The New Oral Anticoagulants: Handle with Care. Philip C. Comp, M.D., Ph.D. October 18, 2013. Speaker for dabigatran (Pradaxa®) and rivaroxaban (Xarelto®). Anticoagulant Quiz. Which commonly used anticoagulant does not require laboratory monitoring? Which anticoagulant has no antidote?

E N D
The New Oral Anticoagulants:Handle with Care Philip C. Comp, M.D., Ph.D. October 18, 2013
Speaker for dabigatran (Pradaxa®) and rivaroxaban (Xarelto®)
Anticoagulant Quiz • Which commonly used anticoagulant does not require laboratory monitoring? • Which anticoagulant has no antidote? • The dose of which anticoagulant depends on renal function? (Enoxaparin, Lovenox®)
The New Oral Anticoagulants Dabigatran (Pradaxa®) Inhibits thrombin Twice a day Atrial fibrillation Apixaban (Eliquis®) Inhibits factor Xa Twice a day Atrial fibrillation Rivaroxaban(Xarelto®) Inhibits factor Xa Once a day Atrial fibrillation; DVT/PE treatment; Reduction in risk of DVT/PE (after 6 mnTx); Hip/Knee prophylaxis;
Canine Model of Blood Coagulation Factor IX Factor X PROTHROMBIN
Canine Model of Blood CoagulationEffect of Warfarin Factor IXa Factor Xa THROMBIN
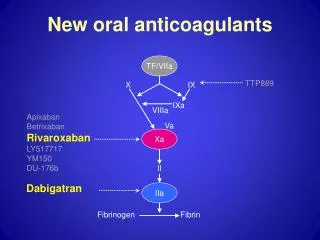
Canine Model of Blood CoagulationOral Anti-Xa Factor IXa Factor Xa THROMBIN
Canine Model of Blood CoagulationOral Anti-thrombin Factor IXa Factor Xa THROMBIN rivaroxaban apixaban
There is no free lunch The effectiveness of an anticoagulant must be weighed against the risk of bleeding Bleeding Thrombosis
Apixaban, Dabigatran and Rivaroxaban • Oral • Short half-lives • Renal clearance • No INRs • No food interactions • Few drug interactions
Prevention of Stroke-Apixaban Number needed to treat/1.8 years: 167 Granger et al. NEJM 3654: 981-92, 2011
Atrial Fibrillation- Dabigatran 35% RRR ! Connolly et al. NEJM 361, 2009 Number needed to treat/ 2 years: 88
Atrial Fibrillation- Rivaroxaban Patel et al. NEJM 365: 883-91, 2011 C Number needed to treat/1.6 years: 135
Atrial Fibrillation- Dabigatran No Treatment CHADS2 Scores 0-1 33% 35% 3-6 33% ESTIMATE 5% risk/year In a non-treated group STROKE Warfarin No Treatment Dabigatran Modified from Connolly et al. NEJM 361, 2009 Number needed to treat NT 88 v. warfarin
Percentage of AF patients with stroke per year No treatment 5.0% Warfarin 1.6% Dabigatran 1.0% ~ 3.4% 100 strokes occur 68% of strokes gone; 32 occur 0.6% 80% of strokes gone; 20 occur Modified from Connolly et al. NEJM 361, 2009
STROKE = Ischemic Stroke and Hemorrhagic Stroke**Subdural hematomas, epidural hematomas, subarachnoid hematomas and intracerebral hemorrhage
Bleeding Event Rate (%/year) N Engl J Med 2011;365:981-92 N Engl J Med 2009;361:1139-51. N Engl J Med 2011;365:883-91.
NNT with dabigatran for 1 year to prevent one adverse event compared to warfarin Nature Reviews Cardiology 7, 10-11 (January 2010)
Can atrial fibrillation studies be directly compared? Mean Age and CHADS2 Score Apixaban 70y 2.1 ± 1.1 Rivaroxaban 73y 3.5 ± 0.94 Dabigatran 72y 2.1 ± 1.1 CHF 1 Hypertension 1 Age > 75 1 Diabetes 1 Prior stroke 2 Direct comparison of strokes and bleeding between studies is difficult.
New oral agents in atrial fibrillation Apixaban superior to warfarin Rivaroxaban not inferior to warfarin Dabigatran superior to warfarin Davis, N Engl J Med 2012;366:1914-22.
Green Tea 333 liters of green tea contain 1 mg vitamin K
New anticoagulants have short half- lives (9-17 hours) Compliance
Forgetfulness 30% Other priorities 16% Decision to omit doses 11% Lack of information 9% Osterberg l et al. NEJM 353: 487-97 2005
1,800,000 patients prescribed a statin: Patients filled prescriptions for a mean of 11.4 medications/3 month 10% of patients filled prescriptions for 23 or more medications. 10% had prescriptions written by 4 or more prescribers. Choudhry NK The Implications of Therapeutic Complexity on Adherence to Cardiovascular Medications. Archives of Internal Medicine 171:814-822, 2011
Retrospective Study of Medication Prescription in Oklahoma City, n=3 • 64 year old man: 14 medications daily; 31 pills • 61 year old woman: 15 medications; 39 pills • 90 year old man: 15 medications; 27 pills
Drugs don’t work in patients who don’t take them C. Everett Koop, M.D. 1916-2013
Who is the ideal patient? • Does not like INRs • Reliable • Well insured
Who will have a bleed? • Frail (<60 kg) • Reduced creatinine clearance • Over 80 years of age Harper. Bleeding Risk with Dabigatran in the Frail Elderly N Engl J Med 2012; 366:864-866
Proper prescriber behavior • At each visit – Are your taking drug X? • At every visit – Why are you taking drug X? • At each visit – Are you taking X every day?
What is the effect of no more INRs? No more anticoagulation clinics and fewer office visits. Will that reduce compliance? BOUNCING BEN in a BAD candidate! INR
Who to switch from warfarin • Not a cure for the bouncing INR • Stroke risk: Least benefit to well controlled warfarin patients • Fewer potential drug interactions in polypharmacy patients?
Warfarin > new anticoagulant Patients angst: Miss INRs Miss food restrictions
If bleeding occurs Little data available a. Factor VIIa b. Factor VIII Inhibitor Bypassing Activity (FEIBA) c. Hydration Fresh frozen plasma and Vitamin K are not the way to go!
Everyone is developing an antidote Oral anticoagulant inhibits factor Xa Inhibitor Xa
Everyone is developing an antidote A recombinant antidote (DU-176b) Xa
Surgery while on medication Dabigatran (100% renal) Rivaroxaban (65% renal clearance) Apixaban (25% renal clearance) When to stop the medication preoperatively depends on the medication and renal function. Look it up!
What is the cost per day* Dabigatran = $9.50 Rivaroxaban= $9.46 Apixaban = $9.40 *Sam's Club, Northwest Highway, OKC 10/10/13
Advising patients • Explain they are taking lots of medications – stroke preventers critical • Avoid friendly little black dogs and get someone else to clean the gutters!
Summary of New Anticoagulants • Marginally better than warfarin for atrial fibrillation • No food interactions; few drug interactions • No need for INRs • Short-half life – take regularly • Check creatinine clearance yearly