Download
1 / 44
440 likes | 1.63k Views
New Oral Anticoagulants Vs Warfain.

E N D
We recommend not commencing anticoagulation in haemodialysis patients with AF just only based on CHADS2 score as in general population, but perhaps those with high risk of thrombotic strokes especially with history of previous strokes.Haemodialysis patients on warfarin should have very close monitoring of INR in dialysis units and the use of heparin for dialysis should be done very thoughtfully. Read attached paper
Arguments: • No blood monitoring is an advantage of NOACs but it is also a major disadvantage. • If good time in therapeutic range, NOACs are not more effective or safer than warfarin. • Phase III clinical trails are not fully representative of real world patients. • Many questions remain around bleeding and peri-operative management.
Aristotle: Subgroup Analysis Read attached paper.
A nephrologist‘s perspective • All AF patients with CHADS2 score ≥2 needs anticoagulant unless there are contraindications. CKD is not an absolute contraindication. Early CKD patents can be treated with either warfarin or new oral anticoagulant (NOAC) as normal population. Just follow Guidelines of international societies. • Late CKD and Dialysis patients are challenging. Risk benefit assessment is important. Warfarin is ok for selected late stage CKD, ESRD and dialysis patients. Limited data on new oral anticoagulant (NOAC) use in this high risk population. • Warfarin Vs NOAC for non-valvular AF or treatment of DVT/PEWarfarin has a notoriously narrow therapeutic window and carries significant risk if not closely monitored. NOAC may be of great use in country like Myanmar because there is no need for monitoring and INR monitoring system is suboptimal. On the other hand, it will be a disaster when there is severe bleeding as no antidote is available and also limited access to special blood products in our country. Antidotes for NOAC are in developmental stage. If available, it will be very expensive for patients in Myanmar. Therefore, it will be a very tough call for clinicians to choose an anticoagulant (warfarin or NOAC) if dialysis patient in Myanmar has AF or DVT/PE. I believe, almost all clinicians in developed countries will choose warfarin in this high risk dialysis patients after careful assessment as evidence on use of NOAC is limited. In valvular AF patients, NOAC is not an effective drug. There and difference in thrombus formation mechanisms between non-valuvular AF and valvular AF. • Nephrotic syndrome patients are unique. They are high risk for thromboembolic disease if albumin <25. As majority of these patients have normal creatinine/eGFR, both warfarin and new oral anticoagulant can be used. But data is limited on use of NOAC and there are reasons why NOAC may not provide adequate protection from nephrotic syndrome associated thromboembolic disease.
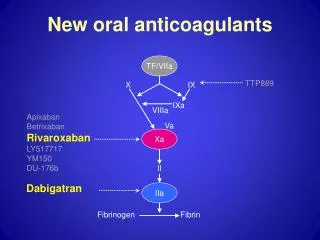
Mechanism of thormbus formation In patients with non-valvular atrial fibrillation, thrombus is formed in the left atrial appendage under low-flow, low-shear conditions in which thrombin generation is believed to be triggered by stasis and endothelial dysfunction. In patients with a valvular AF, coagulation activation and thrombin generation induced by the release of tissue factor from damaged tissues during surgery, exposure of the blood to the artificial surface of the valve leaflets and sewing ring which does not undergo endothelialization for at least several weeks after surgery. • Keys points: • Mechanism of thrombus formation • Selective inhibition of coagulation cascade by NOAC • Non-selective inhibition of coagulation cascade by warfarin • Protein binding ability of drug matters in Nephrotic syndrome patients
Don’t forget the basic Mechanism of thormboembolism A major theory delineating the pathogenesis of venous thromboembolism (VTE), often called Virchow's triad, proposes that VTE occurs as a result of: ●Alterations in blood flow (ie, stasis) ●Vascular endothelial injury ●Alterations in the constituents of the blood (ie, inherited or acquired hypercoagulable state)
Other important Points you should know • Don't forget that warfarin can promote vascular calcification and calciphylaxis. • The routine practice of haemodialysis requires systemic anticoagulation (heparin 500-2000 unit bolus and per hour or clexane 40mg for the whole duration of dialysis) to prevent clotting of dialysis membrane. As INR of 2–3 alone would not prevent fibrin deposition in dialysis membrane, additional heparin is necessary during HD for AF dialysis patients who are taking warfarin.This combination may significantly increase bleeding risk of chronic HD patients but has not been quantified. • On top of that, in-patients receive heparin or clexan DVT prophylaxis on the ward. I am not sure DVT prophylaxis is practised in Myanmar.