Download
1 / 23
280 likes | 537 Views
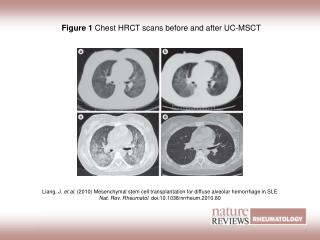
MSCT. Potential Benefits and Limits. Antoine Sarkis, MD Associate Professor of Cardiology Hôtel Dieu de France Hospital. MSCT is a major innovative technique for non-invasive detection of coronary artery stenoses. 129 patients Compare the diagnostic accuracy of multislice CT and MRI

E N D
MSCT Potential Benefits and Limits Antoine Sarkis, MD Associate Professor of Cardiology Hôtel Dieu de France Hospital
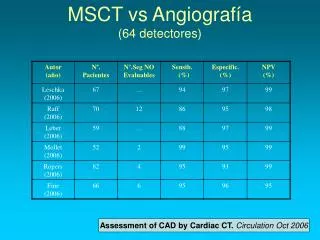
MSCT is a major innovative technique for non-invasive detection of coronary artery stenoses • 129 patients • Compare the diagnostic accuracy of multislice CT and MRI • Sensitivity for detection of clinically significant coronary stenoses (> or =50%): 82 % • Specificity: 90 • Negative predictive value: 95 % Ann Intern Med. 2006 Sep 19;145(6):466-7.
Potential Indications • MSCT in asymptomatic persons • MSCT in highly suspected Coronary artery disease • MSCT in known Coronary artery disease: follow-up of graft patency, stents
MSCT in asymptomatic persons: 1st Scenario: Normal CT • Normal CT in a person with no or minimal risk factors for CAD • Good news, but was-it a surprise? Was the CT really needed?
MSCT in asymptomatic persons:2nd Scenario: Plaque or mild to moderate stenosis • This patient has risk factors, he is asymptomatic, but CT shows ~ 50% stenosis on LAD and RCA. • What is the next step?
MSCT in asymptomatic persons:2nd Scenario: Plaque or mild to moderate stenosis LAD RCA LAD • What is the next step?
MSCT in asymptomatic persons:2nd Scenario: Plaque/or mild to moderate stenosis • This patient had cardiac cath, then cardiac scintigraphy, exactly the inverse classical way of screening asymptomatic patients • He received a total of 36 mSv • Knowing he has multiple risk factors, did CT add information to his status? • Final treatment: Statins, Aspirin, Anxiolytics
MSCT in asymptomatic persons:3rd scenario: severe disease LAD RCA
MSCT in asymptomatic persons:3rd scenario: severe disease • Couldn’t we identify this patient by non invasive testing: Stress test with or without nuclear imaging or echo?
MSCT in asymptomatic persons:4th Scenario: massive calcium 56 yrs old man, smoker, dyslipidemia, hypertension
MSCT as a screning test?Pro • Growing burden of atherosclerotic disease • Known and unknown risk factors • Stess test has limited positive predictive value specially for one vessel disease • MSCT is a cross-sectional imaging technique • It shows the contrast-enhanced vessel lumen (like cath) • It also has the potential to visualize the vessel wall and non-obstructive soft or calcified coronary atherosclerotic plaque • the only clinically available non-invasive study with this capability. • Do it like mammography for cancer screening?
MSCT as screning test?Cons • Come back to the oculo-stenotic reflex? • Does CT add to the information obtained by risk scores based on traditional risk factors? • Could we identify stable plaques, which will stay stable for years, from vulnerable plaques prone to rupture and MI? • CT detects disease, but does it make difference in prognosis? • Cost and reimbursment issues
Best use of MSCT • Patients who have equivocal stress-test results, such as a result that is uncertain or suspected to be false positive or false negative; then the CT is a good test to confirm or exclude coronary disease • Its high negative predictive value suggests it could select patients who should not be referred to conventional angiography, thus avoiding unnecessary coronary angiograms. • CT as a first test should be used only in a selected population, perhaps in patients of younger age in whom the likelihood of having a lot of calcium in the coronaries is low. . . .
MSCT in highly suspected CAD? • Typical chest pain • Positive test for ischemia (Stress test, nuclear imaging) • Little place for MSCT • Go directly to coronary angiography, you can do PTCA in the same time
Follow-up of CABG ? Follow-up of stent placement ? MSCT in known CAD
Limitations • Need to have a relatively slow, regular rythm • Check renal function before injecting Iodine • Problem raised by calcifications • There is still some difficulty identifying stenosis in peripheral segments • Issues raised by high level of radiation
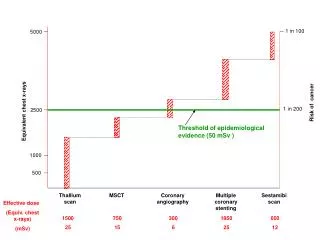
Effective radiation dose from various coronary diagnostic studies • Cardiac Cath = 5-6 mSv. • MSCT = 12-14 mSv. • Calcium scoring scan= 2.6 mSv • SPECT Thallium = 18 mSv. • SPECT Sestamibi = 12.2 mSv. • Normal environment radiation is 3.5 mSv/y. Persinakis, health physics 2002.
Risk of fatal cancer • The International Commission on Radiological Protection (ICRP) has estimated that the additional lifetime risk of fatal cancer is approximately 1 in 20,000 per mSv for the whole population • Based on available estimates, a coronary CT angiogram with an effective dose of 14.7 mSv has a risk of inducing a fatal cancer of 1 in 1,400. • Conventional coronary angiography (5.6 mSv) has a risk of 1 in 3,600 • and a calcium-scoring scan (2.6 mSv) a risk of 1 in 7,700 • We never thought about this risk before !!
ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR Appropriateness Criteria for Cardiac Computed Tomography and Cardiac Magnetic Resonance Imaging • A Report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology Hendel RC, Patel MR, Kramer CM, Poon M. J Am Coll Cardiol. 2006;48:1475-1497.
Report SummaryCardiac Computed Tomography (CCT) • 1. CCT is not appropriate for initial screening of the general population or as an initial tool in evaluation of symptomatic individuals suspected of having coronary artery disease (CAD). • 2. CCT is considered appropriate for evaluation of CAD in patients with prior inconclusive stress test results. • 3. CCT is considered highly appropriate for detection and evaluation of suspected coronary artery anomalies. • 4. CCT is not appropriate for evaluation of bypass grafts and stents in asymptomatic patients • 5. CCT is considered highly appropriate for evaluation of complex cardiac anatomy, especially as related to congenital heart disease.
Report Summary • 6. CCT is considered highly appropriate for evaluation of cardiac masses such as tumor or thrombus, when not ideally evaluated with echocardiographic techniques. • 7. CCT is considered appropriate for evaluation of pericardial disease such as constriction, cyst, or mass when information was not available from echocardiography • 8. CCT with angiography was considered highly appropriate for evaluation of suspected pulmonary embolus. • 9. CCT is considered of uncertain appropriateness for risk stratification prior to non-cardiac surgery.
In conclusion • MSCT will undoubtedly modify our way of thinking • Its place in the screening of asymptomatic persons with multiple risk factors for CAD needs to be defined • Who will resist the temptation of having a look to his coronary arteries by a non invasive technique and without moving one leg ?