Download
1 / 68
700 likes | 744 Views
Carcinoma Oesophagus. DR. B. Ramdas Rai Prof. & Unit Chief YMCH. ETIOLOGY….

E N D
Carcinoma Oesophagus DR. B. RamdasRai Prof. & Unit Chief YMCH
ETIOLOGY…. Alcohol Tobacco Nitrosamines Malnutrition Vitamin deficiency(A,C,Riboflavin) Anaemia Poor oral hygiene Ingestion of hot foods and Beverages
Premalignant conditions… Achalasia Cardia Oesophageal webs Corrosive strictures Reflux esophagitis Hiatus hernia Barrett’s esophagus
Plummer-Vinson syndrome • Leukoplakia • Esophageal diverticula • Ectopic gastric mucosa • Familial ---Tylosis keratosis palmaris&plantaris
Clinical Featrures... Male to female ratio is 3:1 Age:- 6th or 7th decade of life. Recurrent onset of dysphagia is the commonest feature. For the dysphagiato develop, 2/3rd of the lumen should be occluded. Regurgitation Anorexia & loss of weight(severe), cachexia
Contd.. • Pain-substernal or in the abdomen • Liver secondaries, ascites • Bronchopneumonia, malena • Features of broncho-oesophageal fistula in Ca of upper third of oesophagus • Left supraclavicular lymph nodes may be palpable
Contd Hiccough due to phrenic nerve invovement Hoarseness of voice due to involvement of RLN Back pain – due to nodal spread (paraoesophageal/coeliac nodes)
PATHOLOGY • Squamous cell carcinoma—95% • Adenocarcinoma—2.5-5%
SQUAMOUS CELL CARCINOMA • 3 MORPHOLOGIC PATTERNS • Protruded-60%-- • a polypoid exophytic lesion
Flat-15% *diffuse infiltrative form *spread within wall of esophagus *thickening, rigidity, narrowing of lumen
Excavated *necrotic cancerous ulceration *excavates deeply
MOST ARE MODERATE TO WELL DIFFERENTIATED 50% in middle1/3…30% in lower 1/3 20% in upper 1/3
ADENOCARCINOMA • Increasing in frequency • Distal 1/3 • Male : female = 3:1 • Origin---- 1)Barrett’s mucosa 2)Esophageal submucosal glands 3)Heterotropic islands of columnar epithelium
Macroscopically • Appear as FLAT or RAISED patches of otherwise INTACT mucosa • Large nodular masses • Diffusely infiltrative • Deeply ulcerative
Microscopy:: • Mucin-producing glandular . Showing intestinal type feat. • Diffusely infiltrative signet-ring cells of gastric type
SQUAMOUS CELL CARCINOMA • Moderately differetiated
ADENOCARCINOMA • Intestinal type
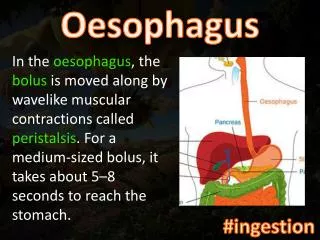
SPREAD Locoregional • Upper1/3 and middle 1/3---tracheobronchial tree ,aorta , left RLN • Lower 1/3---diaphragm, pericardium , stomach
LYMPHATICS • CERVICAL deep cervical paraesophageal posterior mediastinal tracheobronchial LOWER paraesophageal coeliac splenic hilar
Distant spread • Liver • Lungs
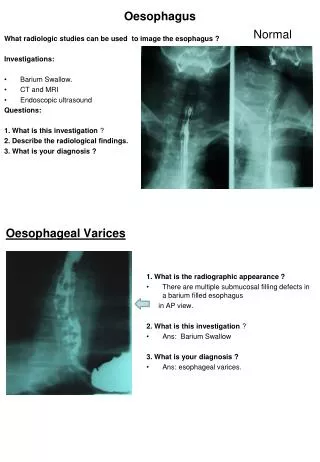
INVESTIGATIONS • Barium swallow • Chest X-ray • Esophagoscopy with biopsy and brushings • CT chest and abdomen • Bronchoscopy
Additional… • MRI • Bone and brain scan • Staging mediastinoscopy if specific symptoms or findings…..
Barium swallow • Irregular mucosal filling defect • Narrowing of lumen at site of lesion • Dilatation proximally
Upper border resembling shelf • Annular lesion—narrowed lumen irregular mucosal outline • Angulation of axis of tumor above and below tumor---spread to extraesophageal sites
CHEST X-RAYS • Air-fluid level in the obstructed esophagus in the postr. Mediastinum • Dilated esophagus • Abnormal mediastinal soft tissue—adenopathy
Pleural effusion • Pneumonitis • Lung abscess • Pulmonary metastasis • CAN BE NORMAL EVEN IN ADVANCED DISEASE
SQUAMOUS CELL CARCINOMA • Protruding • Ulcerating
CT CHEST AND UPPER ABDOMEN • Usually used for staging of the disease • Wall thickness (5mm) • Direct mediastinal invasion by tumor • Regional lymphadenopathy
Metastasis –lung liver adrenal and distant nodes • ESOPHAGEAL ENDOSONOGRAPHY To determine wall penetration and mediastinal invasion—more accurate
BRONCHOSCOPY • Upper and mid esophagus may invade tracheobronchial tree • Positive findings *distortion of bronchial lumen *blunting of carina *intra –bronchial tumor
TNM STAGING • Done using CT • DIVIDES ESOPHAGUS INTO 4 SECTIONS • 1)CERVICAL-15-18cm.lower border of cricoid cartilage to thoracic inlet • 2)UPPER THORACIC—24cm. thoracic inlet to carina
Contd….…. • 3)MIDDLE THORACIC—32cm.carina to ½ the distance to the esophagogastric junction • 4)LOWER THORACIC—40cm.to the esophagogastric junction • REGIONAL LYMPH NODES • CERVICAL --cervical and supraclavicular nodes
THORACIC --mediastinal and perigastric LN along lesser curvature ,fundus,left gastric artery
PRIMARY TUMOR(T) • TX---- can not be assessed • T0 ---no evidence of primary tumor • Tis---high-grade dysplasia • T1 ---invades lamina propria (T1a) muscularis mucosa(T1a) submucosa(T1b) • Does not breach submucosa
T2 ---invades muscularis propria • T3 ---invades periesophageal tissues • T4 ---invades adjacent structures
REGIONAL LYMPH NODES (N) • Nx ---regional nodes cannot be assessed • N0 ---no regional node metastases • N1 ---regional node metastases
DISTANT METASTASIS (M) • Mx ---mets cannot be assessed • M0 ---no distant metastases • M1a ---non-regional lymph node metastases • M1b ---other distant metastases
STAGING • Stage 0---Tis N0 M0 • Stage l--- T1 N0 M0 • Stage lla--T2 N0 M0 T3 N0 M0 Stage llb—T1 N1 M0 T2 N1 M0
Stage lll –T3 N1 M0 T4 any N M0 • Stage lVa –any T any N M1 lVb –any T any N M1b
DIFFERENTIAL DIAGNOSIS • Benign strictures • Benign papillomas • Polyps • Granulomatous masses
TREATMENT • Surgery • Radiotherapy • Chemotherapy • Combination
UNRESECTABILITY • Direct spread to tracheobronchial tree or aorta • Esophageal fistula • Hoarseness of voice • Primary tumor >10 cm.
CHEMOTHERAPY • Combination chemo: • Cisplatin,bleomycin,vindesine or methotrexate
Cisplatin,mitoguazone,vindesine or vinblastine • Cisplatin,5-fluorouracil