Download
1 / 60
630 likes | 1.49k Views
STRICTURES OF THE OESOPHAGUS & CANCCER OF OESOPHAGUS. BY e-mail : elgharma2@yahoo.com Web Site: www.dr-elgharbawi.com Professor MOHAMED A. EL GHARBAWI W. OBJECTIVES.

E N D
STRICTURES OF THE OESOPHAGUS& CANCCER OF OESOPHAGUS BY e-mail: elgharma2@yahoo.com Web Site: www.dr-elgharbawi.com Professor MOHAMED A. EL GHARBAWI W
OBJECTIVES 1.To know types of esophageal strictures 2. Diagnosis & management of corrosive oesophagitis 3. Diagnosis & Treatment of Cancer oesophagus
CAUSES OF OESOPHAGEAL STRICTURES 1) Congenital: Bands, valves with or without tracheo-oesophageal fistula. 2) Traumatic: Foreign body; instrumentation. 3) Corrosive stricture: Multiple long strictures. It is common in children and is usually due to potach. 4) Inflammatory: Non-specific (peptic ulcer) or specific (tuberculosis). 5) Functional: Upper end (Plummer Vinson syndrome) - Lower end (achalasia). 6) Mediastinal tumours: Pressure from the outside. 7) Neoplastic: Benign or more commonly malignant.
CORROSIVE OESOPHAGITIS Aetiology: • Ingestion of corrosive fluids acid or alkalies (soda lime or potash) accidentally in children. • In adults, chemicals may be ingested for suicide. • Acids is less injurious than alkalies
Pathology: • Corrosion is a chemical burn. Its degree depends upon type of fluid and duration of exposure. • Reflex spasm at the lower end of the oesophagus following the swallowing of the corrosive leads to stasis and severe haemorrhagic oesophagitis. • Corrosion causes necrosis of the mucosa and the underlying muscle. • Stricture formation which is multiple and extend from above the level of the aortic arch down to the lower end of the oesophagus.
Clinical features: 1. After ingestion of the corrosive, there is excessive salivation and retrosternal burning sensation. May be dyspnea and stridor 2. The patient may continue to swallow normally for 10-15 days then dysphagia begin to appear. 3. Dysphagia first to solids then, to fluids. Investigations: 1. Barium swallows. 2. Oesophagoscopy: Usually within the first 12 hours of admission.
Treatment: 1. Immediate care: Neutralization of the ingested chemical by suitable neutralizing substance e.g. vinegar for alkalies, sodium bicarbonate for acids and milk for phenol. Care of upper airway passages: e.g. management of laryngeal edema 2. Steroids for 3 weeks to minimize fibrosis.
3. Dilatation (endoscopic): Could be started after the first week, when the acute stage subsides, an attempt should be made to dilate the stricture at oesophagoscopy with a bougie.
4.Operative treatment: Operation is ultimately required in about 40% of cases due to: 1. Complete stenosis. 2. Fistula formation. 3. Failure of dilatation to provide an adequate lumen. 4. Inability of the patient to co-operate with bougienage. 5. Finally, the late development of a carcinoma.
The possible operations are: • Local excision of the stricture if it is short and re-anastomosis. 2. Colon or jejunum interposition or bypass (are the commonest technique to be done). - Some surgeons prefer excision of the strictured esophagus (not by passing), as the strictured esophagus is precancerous. -Preliminary gastrostomy may be needed for feeding to improve the general condition of the patient before the major definitive surgery.
BARRETT’S OESOPHAGUS: • An acquired condition due to gastro- esophageal reflux • It is metaplasia of distal esophageal mucosa • Described by Norman Barrett in 1950 • Distal esophagus is lined by columnar epithelium • May change to dysplasia and adenocarcinoma • Bile reflux appears to be an important etiological factor • 10% of patients with GORD develop Barrett's esophagus • Approximately 1% of patients with Barrett's esophagus per year progress to carcinoma • Barrett's esophagus increase the risk of cancer by x30
BARRETT’S OESOPHAGUS: Clinical features • Usually asymptomatic • Usually an incidental finding at endoscopy • Appears as 'velvety' epithelium extending more than 3 cm above gastro- esophageal junction • The significance of 'short segment' Barrett's (<3 cm long) is unclear
BARRETT’S OESOPHAGUS: Management • If diagnosed at endoscopy most patients are started on life-long acid suppression • Little evidence exists that it causes regression of metaplasia • Anti-reflux surgery may reduce progression to dysplasia and cancer • Recent interest has been shown in endoscopic mucosal ablation • Usually achieved with photosensitizers and laser therapy • The role of endoscopic surveillance of Barrett's esophagus is controversial • Aim of surveillance is to detect dysplasia before progression to carcinoma • 40% patients with dysplasia have focus of adenocarcinoma • Oesophagectomy for dysplasia has an 80% 5-year survival
CARCINOMA OF THE OESOPHAGUS Incidence: • Age: Common >50 years of age. • Sex: Males >females, except in cervical esophagus. • 90% are squamous cell carcinomas Occur in the upper or middle third of the esophagus • 8% are adenocarcinomas Occur in the lower third of the esophagus • Overall 5 year survival is very poor and is at best 20% • < 50% patients are suitable for potentially curative treatment • Of those undergoing 'curative' treatment less than 40% survive one year
OESOPHAGEAL CARCINOMA Predisposing (RISK) factors: Squamous cell carcinoma • Cigarette smoking. • Alcohol intake. • Achalasia. • Leukoplakia. • Diet high in nitrosamines • Trace element deficiency – molybdenum • Vitamin deficiencies - vitamins A & C • Coeliac Disease Adenocarcinoma • 15% associated with Hiatus hernia and reflux with Barrett's oesophagus.
Pathology: 1) Site: Upper third 20%. Middle third 35%. Lower third 45%. 2) Gross appearance: a. An annular stenosing lesion. b. An epitheliomatous ulcer with raised everted edges. c. Rarely fungating friable mass.
3) Microscopically: a. Squamous cell carcinoma: The commonest. - Differentiated. - Undifferentiated, formed of packed masses of cells. b. Adenocarcinoma. In the 1/3 , originated from: - Extension from the cardiac end of the stomach. - Ectopic gastric mucosa. - Arises from Barrett's oesophagus. c. Basal cell carcinoma: Rare.
4) Spread: a. Direct: The main method of spread. It is both transverse and longitudinal in direction. It erodes the muscular wall to invade important structures such as: Bronchus and mediastinum, aorta, and the left recurrent laryngeal nerve causing hoarseness of voice. b. Lymphatic: - Cervical oesophagus: drains to lower deep cervical lymph node and superior mediastinal lymph node.
- Thoracic oesophagus: Tracheo-bronchial lymph node and posterior mediastinal lymph node. - Abdominal oesophagus: Coeliac lymph node. Submucous lymphatic permeation may lead to nodules away from the main tumour. c. Blood: Liver and lungs. 5) Complications: 1) Progressive cachexia. 2) Mediastinitis. 3) Erosion of aorta. 4) Pneumonia. 5) Hoarseness of voice.
Clinical picture 1. Dysphagia: - Course: Progressive. - Duration: Short. - First for solid more than fluid: later for both. -Later patient can't swallow his own saliva. 2. Regurgitation. Due to overspills of saliva. 3. May lead to respiratory symptoms especially with tracheo-oesophageal fistula 4. Retrosternal pain due to: -Involvement of nerves. - Secondary infection. 5.Bleeding (rare). 6. Cachexia (weight loss).
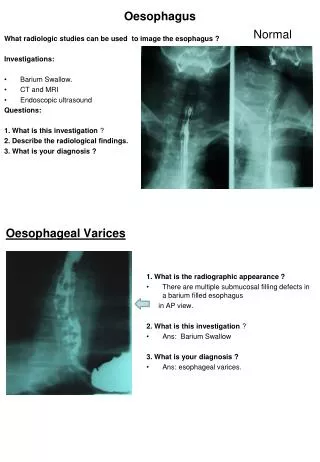
Investigation & Assessment: 1) Barium swallow: - Irregular filling defect. - Long segment of stricture with shouldering and mild oesophageal dilatation above (rat-tail appearance). 2) Oesophagoscopy: - Diagnostic (type, level). - Biopsy: Direct and brush cytology.
BARIUM SWALLOW, NORMAL & CANCER OESOPHAGUS
3) Investigation to evaluate its spread: - Bronchoscopy: To detect invasion in the trachea and in the bronchi. - Indirect laryngoscope: For vocal paralysis. - Venous azygography: For mediastinum invasion. - CT chest and abdomen for extent of spread. - Endosonography for local spread. - Ultrasonography: For liver metastasis.
D.D.: Between Achalasia and Carcinoma of Oesophagus
BARIUM SWALLOW, ACHLASIS ACHALASIA ACHALASIA, HEN’S Peak
BARIUM SWALLOW, CANCER OESOPHAGUS CANCER OEOPHAGUS Middle 3rd CANCER OESOPHAGUS lower 3rd RAT TAIL
TREATMENT OF CANCER OESOPHAGUS • Adenocarcinomas are not radiosensitive and surgery is mainstay of treatment • Squamous cell carcinomas can be treated with either surgery or radiotherapy • Cancer esophagus is treated by surgery, radiotherapy, or combinations of both. • Operable cases are treated surgically • Only 40% tumors are resectable • Operative mortality now less than 10% • Treatment should be in centers performing operation regularly • No place for the occasional operator • Preoperative radiotherapy may be beneficial
Resectability & fitness for surgery assessed by: • Chest x-ray • Lung function tests • Liver ultrasound • Endoscopic ultrasound • Bronchoscopy • Laparoscopy • Thoracic CT Indication of in-operability: local or distant spread lung involvement phrenic nerve paralysis vocal cord paralysis involvement of mediastinal lymph node.
TREATMENT OF CANCER OESOPHAGUS A.Surgery for Operable tumors: • Surgery is to excise the oesophagus 2 inches above the tumor and down to stomach. • Replacement of excised oesophagus is done by different methods (gastric pull up, colon interposition…. etc.) the commonest technique to be done is to mobilize the stomach up in the chest and anastomose it with remnant of proximal oesophagus.
The approach for oesophagectomy • Need 10 cm proximal clearance to avoid submucosal spread. • Total oesophagectomy via thoracoabdominal approach (Adenocarcinoma) • Subtotal two-stage oesophagectomy (Ivor-Lewis) • Subtotal three-stage oesophagectomy (McKeown) • Transhiatal oesophagectomy Differs according to site of the cancer: (1)Tumor of lower third: Limits of resection: Partial oesophago-gastrectomy (excision of oesophagus 2 inchs above the tumor and the upper part of the stomach) . N.B.: Spleen and tail of pancreas are usually included in the resection. Drainage pyloroplasty may be added as the vagus nerve is excised.
Surgical approaches: The tumors of lower third (partial oesophago-gastrectomy) could be done through: a- Left thoraco-abdominal incision. or b- Upper midline abdominal + Right Thoracotomy in 5th intercostal space (Ivor -Lewis procedure). Continuity is restored by anastomozing remnant of the oesophagus to stomach in the chest (gastric pull – up).
(2)Tumor of middle third (and thoracic part of upper third): Limits of resection: Subtotal oesophagectomy (removal of oesophagus 2 inchs above the tumor and down to the cardia). Surgical approaches: a) Same approach of Ivor – Lewis procedure, mentioned above.
b) Nowadays, many surgeons prefer to do total oesophagectomy through a transhiatal approach (abdominal) without thoracotomy + cervical approach to anastomose stomach to cervical oesophagus in the neck. This approach is much safer, as if anastomotic leakage occurs, it will be away from the chest.
(3)Tumor of upper third (cervical part): Limits of resection: Total oesophagectomy down to cardia ± pharyngo-laryngetomy ± Radiotheray Approachs: Through abdominal approach + cervical approach through an incision along the anterior border of left sternomastoid. The excised oesophagus could be replaced by colonic or jejunal graft .