Download

1 / 17
170 likes | 192 Views
Explore the impact of malaria on transfusions, recent cases, standardisation proposals, and replacement of HBV and HCV DNA standards. Learn about screening methods and candidate P. falciparum standards. Collaborative studies and data comparisons are also discussed.

E N D
Standardisation of P. falciparum HBV, HCV and NAT Sally Baylis, NIBSC SoGAT XVIII
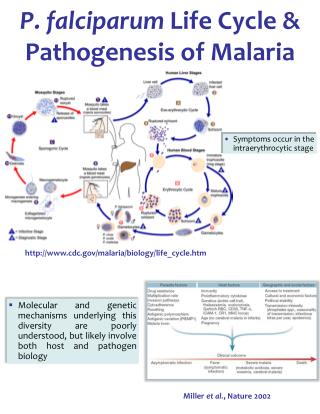
Malaria • 300 to 500 million cases annually (1.5 to 2.7 million deaths) • 4 plasmodia species cause malaria in man • Plasmodium falciparum causes ~80% of cases (malaria tropica) • P. vivax (~15% cases) , P. ovale, P. malariae less severe • Transmitted by night-biting Anopheles mosquitoes • Complex lifecycle with species variation • Asexual in man • Sexual in mosquito
Malaria cont. • In non-immune host e.g. visitors to endemic areas • Incubation period normally 1-3 weeks • Seroconversion up to 4 months after infection • Symptoms - fever, chills, malaise, headaches etc. • In the semi-immune host e.g. immigrants & visitors from endemic areas, those taking prophylaxis • Delayed onset of illness & mild symptoms • In the “immune” host • Malaria is less severe & asymptomatic in 80% of individuals
Malaria and Transfusion • Transfusion-transmitted malaria is rare, but potentially serious consequence of blood transfusion • US, ~ 90 cases since 1963 • Canada, 3 cases (1994-1999) • UK, 5 cases in last 15 years • Generally prevention of transfusion transmitted malaria by donor selection to identify those “at risk” e.g. • Born/ lived in endemic areas • Visitors to endemic areas • Had malaria
Malaria and Transfusion cont. • Most recent UK case of transfusion transmitted malaria in 2003 (Kitchen et al., Vox Sang. 88, 200-1) • Recipient: • Male (age 50) with sickle cell disease & renal failure became symptomatic ~ 2 months after transfusion • Blood films – P. falciparum trophozoites; 5.2% parasitaemia • No history of travel outside UK since 1957 • Donor: • Female (age 38) from Ghana, migrated to UK & not returned to Ghana in previous 8 years • No history of malaria • Malaria Ab EIA positive serum archive sample (Newmarket) • Follow up blood samples from donor, malarial ab +ve & P.falciparum DNA was detected by qPCR (~5 parasites/μl - 8 months post-donation; 0.0005 parasites/μl - 12 months post-donation)
Screening for Malaria • Deferral & antibody screen for donor reinstatement e.g. the UK – Newmarket EIA; US no approved tests • However will not detect “window” • Stained blood films – routine method for diagnosis (since 1900) • Slow, requiring highly trained microscopists • Antigen detection • Lacking in sensitivity • Nucleic Acid Detection • Potentially may not detect very low levels of parasitaemia
NIBSC Proposal for Production of Standards for P. falciparum For standardisation of NAT assays (qualitative and quantitative) Screening of blood for transfusion and tissues: exclusion of infected donations (run controls); determination of levels of parasitaemia where TTIs occur; validation of assay sensitivities Diagnosis and clinical management of malaria: standardisation of commercial and in-house tests – harmonisation of results to a single reference material Vaccine studies: cross-comparison of studies, parasite loads, efficacy etc.
Candidate P. falciparum Standards • Freeze-dried blood from patient (~10% parasitaemia) • Liquid preparation of blood from patient (~7% parasitaemia) • Liquid preparation of P. falciparum cultured in vitro to ~10% ring forms • Liquid preparation of blood from patient (~0.007% parasitaemia)
Performance of Candidate Freeze-Dried P. falciparum Standard • No significant loss of titre is observed following freeze-drying of patient blood (~10% parasitaemia) • Accelerated degradation studies of this material are in progress • >8 months at -20 ºC, no change in titre
Collaborative Study • Commenced April 2005 • 9 laboratories already received samples • 3 further laboratories are finalising receipt details • Labs wishing to participate in the collaborative study should return form in meeting pack to S. Baylis
Replacement of the HBV DNA IS 97/746 The 1st International Standard for HBV DNA was established by the WHO ECBS in October 1999 Estimated date of exhaustion of the IS will be 2006 at current rate of usage Materials coded AA (97/746) & BB showed no significant difference in potency in the collaborative study ECBS noted that BB (made from the same stock as AA) could be reserved for potential future use as a replacement standard
Replacement of the HBV DNA IS 97/746 cont. • Additional stability studies required before BB able to replace AA • Propose small collaborative study, similar to that of the HCV RNA IS replacement • Aim to demonstrate the equivalence of the candidate replacement (BB) to AA • Real-time data on AA and BB samples • Accelerated degradation data on AA and BB • Aim to submit report to WHO ECBS by July 2006
Replacement of the HCV RNA IS 96/798 Approximately 1250 vials remain of the 2nd HCV IS 96/798 Estimated date of exhaustion of the IS will be 2009 at current rate of usage Options for replacing the IS 1st & 2nd IS derived from the same genotype 1a anti-HCV positive donation Do we replace the IS with a donation positive for anti-HCV or negative for anti-HCV? 1st & 2nd IS diluted in cryosupernatant Do we dilute a replacement IS in cryosupernatant or plasma?
Acknowledgements David Padley, Alan Heath & Nita Shah, NIBSC Peter Chiodini, Hospital for Tropical Diseases, London Patricia Hewitt, NBS, London Claire Swales, LSHTM, London