Download
1 / 25
250 likes | 258 Views
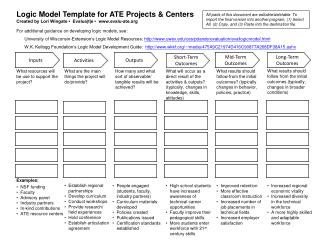
Middle- term outcomes of an original procedure of ligamentoplasty for chronic lateral instability of the ankle. J.P. Marchaland, L. Matthieu, A. Bouchard, Y. Nader, C. Bures, L. N’Guyen, G. Versier. Military hospital Begin- Saint Mandé- France. MATERIAL AND METHODS. Retrospective Study

E N D
Middle- term outcomes of an original procedure of ligamentoplasty for chronic lateral instability of the ankle. J.P. Marchaland, L. Matthieu, A. Bouchard, Y. Nader, C. Bures, L. N’Guyen, G. Versier. Military hospital Begin- Saint Mandé- France
MATERIAL AND METHODS Retrospective Study 36 patients operated between 2002 and 2005 Ratio : 1 ♀ / 7 ♂ Middle age : 28 years [18 – 36 years] • Chronic lateral instability < 5 sprains : 6 % 5-10 sprains : 40 % > 10 sprains : 54 % • Contra lateral instability : 25 %
MATERIAL AND METHODS • Hyper laxity : 40 % • Sub talar instability : 6 % • Average differential varus (stress X-Rays) at pre operative time: 4,8° [-3° à 15°] • Tibio talar arthritis: 0 • Pain (n=8) MRI : 8 lesions of the CLL 2 lesions of the TCL (Sub talar instability) 0 osteochondral defects of the talus • Time surgery/ 1st sprain: 84 month [12 – 180 month]
MATERIAL AND METHODS Surgical technique • Supine position, tourniquet • Lateral approach 1- Ligamentoplasty “Castaing like” - A half peroneus brevis (8 cm) crossing through a - Malleolar Tunnel (Ø 4,5) - Create a loop and - Suture on itself at the metatarsal basis insertion
2- Tightening of the antero- lateral capsule “Duquennoy like” - Detachment of the antero- lateral capsule - Articular exploration - Trans osseous attachment (Malleolar Tunnel (Ø 2) or anchors)
Sub talar instability(n=2) - Scraping out of the tarsal sinus (TS) - Capsular plasty of the TS + Plasty with the extensorum digitorum brevis (Pr. MOYEN) Post operative cares : - Below knee cast for 45 days - Proprioceptive rehabilitation - Return to sports : 4 to 6 months Complications:especially - 4 skin disorders (healing problem) - 3 algodystrophy 21,4 %
MATERIAL AND METHODS Revision • Profession and sports (C.L.A.S.) • Subjective assessment • Ankle scoring system of MOLANDER and OLERUD (100 pts)
Revision(suite) • Clinical exam: foot morphology, motion, hyper laxity, pain • Bilateral peroneus brevis strength measured with a dynamometer(Strength in eversion) • Stress X-rays (varus laxity of the both ankles): differential varus Strength in eversion 3 measures- Same examiner Stress X- Rays
MATERIAL AND METHODS Statistics Epi-Info version 6.04 distributed by ENSP- Rennes ( Center for Disease Control, USA) : comparative analysis with Khi2 test Fischer test if data < 5
RESULTS •28 patients reviewed Revision rate : 78 % 4 bilateral surgery = 32 ankles •Follow-up : 20 months [6- 64] •Recovery of job :100 % 78%: job with risks of sprains
RESULTS •Recoveryof sports : 97 % Sport level • Pre operative • Revision - 1 patient stopped - 3 patients level : C L
Pre operative n= 29 • Revision n= 28 Sports • Team sports (soccer, basket ball, rugby) • Running
RESULTS •Subjective assessment 91% satisfied and very satisfied •Cause of dissatisfaction • Pain (21%) • Stiffness (15%) • Apprehension (6%) • Complications (3%) No recurrence of sprain
RESULTS •Clinical exam - Foot morphology normal : 91 % hind foot varus : 9 % - Dorsal flexion Operated side : 17,5° [10°-25°] Healthy side : 18,6° [10°-25°] - Plantar flexion Operated side: 43,3° [30°-55°] Healthy side: 46,6° [30°-55°] No significative difference No significative difference
RESULTS •Ankle score Revision : 91,5 [70 – 100] versus Pre operative : 56,8 [30 – 85] p < 0,05
RESULTS •Strength in eversion • Operated side: 17,5 kg [11-20] • Healthy side: 18,5 kg [12-23] Loss of 5 % = NS • Differential varus • Pre operative: 4,8° [-3° à 15°] • Revision: 0,6° [-9° à 5°] p < 0,05 • Tibio talar Arthritis : 0
ANALYTICAL RESULTS •Satisfaction Less good (p<0,05) - pain - stiffness - loss of strength No influence - age - activities (sportsmen vs sedentary) - sport level
ANALYTICAL RESULTS •Ankle score Diminished(p<0,05) - Age (> 28 years) - Complications (pains) - Stiffness No influence - Nb of sprains before surgery - Apprehension - Activities (p=0,06)
ANALYTICAL RESULTS •Feeling of stiffness • plantar flexion (p<0,05) • ankle score (p<0,05) • No correlation • Differential varus at revision •Hind foot in varus No correlation - apprehension - pain (p=0,08)
DISCUSSION • Ligamentoplasty of CASTAING[1,2] Advantage : durable effectiveness +++ Disadvantage : stiffening of the sub talar joint (sportsmen) sacrifice of peroneus brevis • Tightening of DUQUENNOY[1,2] Advantage : diagnostic and therapeutic arthrotomy +++ Disadvantage: progressive pulling 1- Kouvalchouk JF, Hassan E. Chirurgie des laxités chroniques latérales de la cheville. Encycl Méd. Chir (Elsevier, Paris), Techniques chirurgicales – orthopédie traumatologie, 44-901, 1998. 2- Besse JL. Traitement des entorses graves et instabilités chroniques de la cheville. Cahiers d’enseignement de la SOFCOT 1997, 62 : 187-217.
DISCUSSION • Recovery of activities • Subjective results • Functional results Comparable with SOO 2005[3] : 3- Dubrana F. Symposium de la SOO sur l’instabilité chronique autour de la cheville. Rev Chir Ortho 2006, 92, 1S11-1S40
DISCUSSION Comparable with other techniques[2] : Karlsson [4] Roy-Camille [5] Ligamentoplasties with PB: - Chrisman-Snook [6] - Watson-Jones [7] 2- Besse JL. Traitement des entorses graves et instabilités chroniques de la cheville. Cahiers d’enseignement de la SOFCOT 1997, 62 : 187-217. 4- Karlsson J et al. Reconstruction of the lateral ligaments of the ankle for chronic lateral instability. J Bone Joint Surg 1988 ; 70A : 581-588 5- Roy-Camille R et al. Les laxités externes chroniques de cheville. Rev Chir Orthop 1986, 72, 121-6 6- Bernhard JA, Burckhardt A. Long term results following fubulo-tarsal ligament reconstruction. Swiss Surg 1996, 2(6) : 274-9. 7- Colombet P et al. Traitement de l’instabilité chronique de cheville par la technique de Chrisman Snook. Rev Chir Orthop 1999, 85 : 722-726.
DISCUSSION • Problem: complications : 21,4% Scars disorders No sub cutaneous detachment in the approach ! Algodystrophy Decrease time of plaster cast(3 weeks) SOO 2005 [3] 131 Hemi-CASTAING : 22 % 10 algodystrophy, 8 Achilles tendinitis, 6 nevromas, 2 peroneus tendinitis, 2 infections 76 DUQUENNOY : 5 % 2 scars disorders, 1 infection, 1 algodystrophy, but 5 recurrences … 3- Dubrana F. Symposium de la SOO sur l’instabilité chronique autour de la cheville. Rev Chir Orthp 2006, 92, 1S11-1S40
DISCUSSION • • Stiffness • Lesser functional result • Ability of stretching of PB < Collateral lateral ligament [2] • Over correction? - no correlation with differential varus, but statistical trend (p=0,06) - keep a small varus 2- Besse JL. Traitement des entorses graves et instabilités chroniques de la cheville. Cahiers d’enseignement de la SOFCOT 1997, 62 : 187-217.
CONCLUSION • Original set of patients (military): sports +++ • Very good functional results • No recurrence • Frequent stiffness Do not tighten too much the graft !