Download
1 / 31
320 likes | 577 Views
Patient Preference and Comprehensive Cohort Designs. Background. Patients often have a preference for treatment. Patients with strong preferences for ‘usual care’ often do not get into a trial because randomisation does not guarantee that they will get what they want.

E N D
Background • Patients often have a preference for treatment. Patients with strong preferences for ‘usual care’ often do not get into a trial because randomisation does not guarantee that they will get what they want. • Patients who do get into a trial with strong preferences for the ‘novel’ treatment can bias results.
Strong preferences • When a treatment is ONLY available within a trial context patients who want the treatment may decide to consent to randomisation with the hope they may get the treatment. • This can lead to the following problems: • Demoralisation • High drop out • BIAS
Effect of Preferences • Patients may refuse to fill in follow-up questionnaires due to ‘resentful demoralisation’, which can lead to bias. • Patients who DO get what they want may ‘exaggerate’ the effectiveness of their treatment – again this MAY lead to bias.
Quality of Life and Preference • Preferences are particularly a ‘problem’ when quality of life is a major outcome as this is more susceptible than objective measures of outcome (e.g death).
Patient Preference Trial – A solution • One approach to the issue of preferences is to undertake a ‘patient preference trial’. • Only patients ‘indifferent’ to which treatment they receive are randomised. • Trial also known as ‘Brewin-Bradley or Comprehensive Cohort Design’.
Preference Example • A trial of two methods of abortion – medical termination (mifepristone) vs surgical aspiration. • Some women had strong preferences and therefore were allowed their treatment choice.
Abortion Trial Heshaw BMJ 1993;307:714-7.
Data from Abortion Study • The extra benefits of the preference study showed that clinically there was no difference. • HOWEVER, women with a preference should be allowed their choice women who were indifferent with late gestation would find surgical abortion more acceptable.
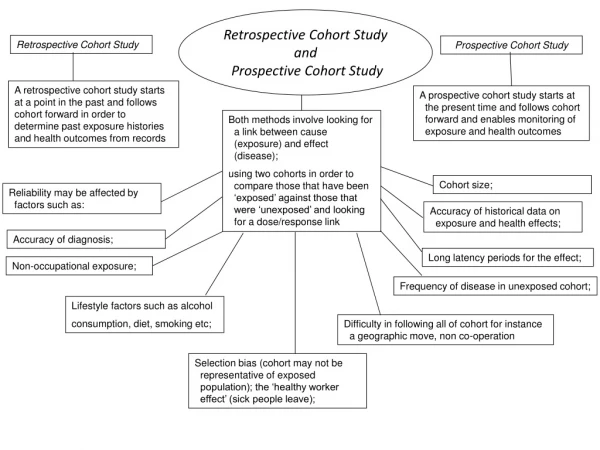
Comprehensive Cohort • In a comprehensive cohort study, Porthouse looked at the fracture rates among women who took part in a fracture prevention trial compared with those who were either ineligible or would not participate.
Comprehensive Cohort Design Source: Porthouse: MSc thesis and QJM 2004;97:569.
Results • Those taking part had significantly lower risk of fracture compared with similar, eligible, women refusing to take part. • Recruitment to fracture prevention trials selects individuals who are at lower risk than those for whom the treatments will eventually be used.
Problems with Preference Design • Because preference arms are not formed by randomisation they WILL be exposed to selection bias. • This makes the comparisons of these arms hazardous.
Preference Recruitment • Trial recruitment is unaffected by the inclusion of preference arms EXCEPT for the extra resources needed to follow-up the preference arms. • Cooper et al. undertook a RCT of the preference design and found no advantage to it. Cooper et al. Br J Obs Gynae 1997;104:1367-73.
An Alternative? • One approach to preserve the benefits of randomisation is to undertake a fully randomised preference trial. • ALL patients would be randomised irrespective of their preferences and preference would be used in the analysis. Torgerson et al. 1996;1:194-7.
Example • York Back Pain trial randomised 187 people with low back pain to an exercise programme or control (benign neglect?). • Before randomisation patients were asked their preferences. • 63% expressed a preference for the new treatment 37% had no preference.
Backpain Preference Trial Klaber Moffett et al. BMJ 1999;319:279-83.
Back Pain Trial • In the back pain trial we were able to show that the intervention was just as effective among patients who were ‘indifferent’ to having the exercise therapy compared with those who were really ‘keen’.
Antenatal Care • In a trial of increased visits to women for antenatal care it was found that women with a strong preference for the alternative were much more dissatisfied with treatment.
Antenatal Trial – Dissatisfaction with Treatment Clement et al. 1998 BMJ 317:78
The most interesting example • SPRINTER is an RCT of treatments for neckpain. • Two treatments: a Brief Intervention (1-2 sessions with a physio using CBT) vs usual care (5+ sessions). • BEFORE randomisation we asked patients their treatment preference.
SPRINTER Preferences • In SPRINTER preferences were mixed • 53% did not have a preference; • 16% wanted brief intervention; • 31% wanted usual care. • ALL patients were randomised IRRESPECTIVE of their preference.
Patient Flow and 12 month Results - SPRINTER Overall 12 month improvement -0.840 Overall 12 month improvement -2.825
SPRINTER interpretation • Had we not asked for preferences we would have concluded usual care is best for all. • BUT we can now say that BI is best for those who want that treatment (also much cheaper) and UC should be reserved for those who want it or ‘indifferent’ patients.
Where now preference? • In MY view if there is likely to be a problem with preferences we should elicit these at the start of the trial and include them in the analysis. • Patient preference trials of the Brewin-Bradley design are fraught with analytical problems – selection bias.
Doctor Preference • As well as patients one could use doctor preferences to allocate treatment. • In a RCT of orthopaedic surgery vs orthopaedic medicine patients were only randomised if GP was indifferent to the specialist needed. • Patients with a named consultant were included and followed. Leigh-Brown et al. 2001 Health Bulletin 59;198-210.
Doctor Preference • In the OMENS trial Leigh-Brown et al found that outcome did not seem to be affected by physician preference. • Outcomes were similar across groups with orthopaedic medicine being more cost effective.
Summary • Patient preferences CAN affect outcome. • Elicitation of preferences when this is an issue BEFORE randomisation can be important.