Download
1 / 29
290 likes | 406 Views
Hard to swallow. Dysphagia Awareness Training For Care Homes. Course objectives. By the end of this workshop, you will: Have an understanding of dysphagia, what can cause it and what the risks are Be able to identify when someone has a swallowing problem and know what first actions to take

E N D
Hard to swallow Dysphagia Awareness Training For Care Homes
Course objectives • By the end of this workshop, you will: • Have an understanding of dysphagia, what can cause it and what the risks are • Be able to identify when someone has a swallowing problem and know what first actions to take • Know when and how to refer to SLT • Be able to support a resident with dysphagia to eat and drink as safely and comfortably as possible.
CQC requirements & dysphagia • Some of the CQC regulations that are relevant for dysphagia: • Supporting residents to eat and drink enough and maintain a balanced healthy diet • Coordination of care with other professionals such as SLT and Dietetics • Identifying needs and risks around swallowing • Supporting people in a sensitive manner to meet their nutritional requirements, taking the resident’s own views and wishes into account • Effective care based on best practice from staff who have the knowledge and skills to carry out their roles and responsibilities
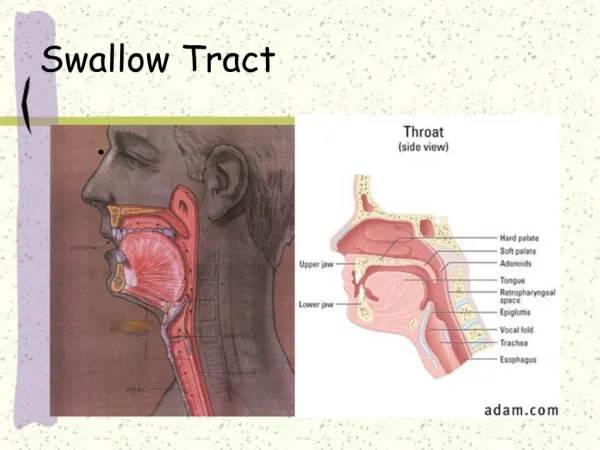
Normal swallowing vs. dysphagia • Dysphagia = a disorder of swallowing • Swallowing is the movement of food, drink and saliva from our mouth to our stomach without letting it enter our airway • Normal swallowing is a complex process that we do around 1500 times per day, even when we’re asleep • Swallowing is partly under our control and partly a reflex • For this workshop we are talking about ‘oropharyngeal dysphagia’ – this is the part of the swallowing process that SLTs are expert in and can assess and advise on • Animation clip of normal swallowing: https://www.youtube.com/watch?v=eLvfzyZNnVw
Understanding dysphagia • What can go wrong with swallowing? • Anything! The swallow can break down anywhere and usually in more than one part of the process • Dysphagia can present in many ways. It can be: • Transient (short term) • Fluctuating (better and worse at different times) • Persistent/chronic (long term) • Deteriorating (gradually getting worse)
What else can make swallowing more difficult? • Feeling drowsy or less alert • Reclined or lying down • Distracted • Talking while food is in the mouth • Partial / no dentition, loose dentures, dentures not in • Over filling your mouth • Eating too fast • If any of these things are difficult, then the risk of unsafe swallowing is higher.
Dysphagia – what are the risks? • Aspiration • Small amounts of food/drink/meds go into airway and lungs instead of oesophagus (food pipe) + stomach • Can be noisy with coughing, or sometimes silent (no coughing) • Can cause chest infections and pneumonia. • Choking • Airway is blocked with solid food, risk of sudden death. • Inadequate nutrition and/or hydration • Harder to eat and drink enough, sometimes reluctance to eat or drink. • Social and emotional impact – embarrassment, less involved in social meals, drinks etc, less enjoyment of food & drink, impact on choice and independence, anxiety and distress.
Dysphagia: identification • What are the signs and symptoms of dysphagia? • Coughing/spluttering on food/drink • Choking • Drooling • Wet gurgly voice, especially after food/drink • Frequent chest infections/aspiration pneumonia • Pocketing food, residue in mouth • Holding food in mouth for long periods • Person complains of difficulty • Complains of food getting stuck going down (* NB this often suggests a difficulty lower down, in the oesophagus/food pipe) • Less likely: refusing food/drink, pain on swallowing, reduced appetite
Identifying a swallowing problem – first steps • Observe and document any difficulties – is there a pattern? • Check if there is any history of dysphagia • Has the resident seen SLT before? What were the most recent SLT recommendations? • Check that the resident is on the correct diet and fluids as recommended by SLT • Put in place extra measures to make swallowing as safe as possible • Monitor closely and document your observations • Think about whether you need to make a referral to SLT for a full specialist assessment of swallowing
When a resident needs help with feeding • The way we eat and drink is very individual • Temperature – lukewarm tea, anyone? • Meat first, then veg – or a little bit of everything on the fork? • Custard on everything, by the side or not at all? • Small sips or big gulps? • When we need someone to feed us, we lose that control • How would that feel?
Top tips for safer swallowing (1) • Make sure that: • The person is fully alert and awake for anything that they need to swallow (food, drinks or medication) • The person is sitting as upright as possible with their chin slightly down • You have checked that the most recent SLT swallowing advice for this resident is being followed • Help is available for the person to feed themselves. Encourage the person to concentrate and not to talk while they are eating
Top tips for safer swallowing cont’d (2) • Make sure that: • Mouthfuls or sips are not too big. • Eating and drinking is at a steady rate and not too fast. Watch for a swallow and a clear mouth before the next spoonful or sip is taken • (These last two things are much harder if someone else is feeding you) • Check that utensils are really needed • Check that their mouth is clear after each meal • Good oral hygiene is maintained by regular mouth care.
Risk factors to be aware of • Choosing the right moment could make a difference • Alertness/cooperation • Distractibility • Fatigue • Supporting someone’s general health could make a difference • Seizure activity • Oral health problems • Underlying respiratory problem • Posture control • Unmanaged pain • Mental health problems • Medication • Injury/discomfort • If you are aware of these things, it could make a difference • Level of learning disability/cognitive function • Rapid decline in function due to ill health (decompensation) • Behavioural difficulties • How you manage the care environment and support could make a difference • Physical environment • Social environment • Access to specialised equipment • Staffing level • Staff adherence to a plan • Quality of life/loss of dignity
When to refer to SLT • If there are signs of a new swallowing difficulty or if swallowing problems have got worse • If the problem seems to be at the mouth and throat level (oropharyngeal) and not lower down (oesophageal) • If you have not been able to manage the swallowing difficulty by putting in place basic safer swallow measures, eg. making sure that they are alert and upright. • NB If the person has been seen by SLT in the past and has a plan in place for eating and drinking at risk, then discuss with SLT before re-referring.
If the person also has a learning disabilityyou can also refer • To screen the person for swallowing difficulty – ‘just to check’ • Refusing to eat/drink – this usually relates to appetite or cognition and not swallowing • Too drowsy/unwell to eat/drink • Pain on swallowing – needs examination by doctor • Vomiting/regurgitating/food sticking at oesophageal level • See SLT handout “Swallowing Difficulties or Dysphagia in Care Homes” for more information
How to refer to Adult SLT • Complete our referral form with as much relevant information as possible • Send via secure email to our central point of access: kentchft.aslt@nhs.net We cover these areas: • Ashford & South Kent Coast • Canterbury & Coast • Thanet • West Kent • We will then process the referral by triaging and prioritising by clinical risk and referral date.
How to refer to LD SLT • Complete our referral form with as much relevant information as possible. • You can do this on paper, or fill in the online version by visiting the learning disability KCHFT website pages. • or call us if you have any queries or urgent concerns. • Send the forms to our central point of access:kentchft.ldsref@nhs.net or snail mail to the address at the top of the form. We cover these areas: • Ashford Canterbury and Coastal • South Kent Coast and Thanet • Dartford, Gravesham, Swanley and Swale • West Kent
Managing dysphagia • We aim to: • Maximise health and well-being • Minimise risk of aspiration and choking • Minimise risk of under-nutrition or dehydration • Keep someone eating and drinking for as long as possible with as few restrictions as possible • Give clear information to the patient, family/carers and other health professionals about the swallowing problem • Sometimes dysphagia can be treated and swallowing can be improved, eg after a stroke. Often it is not possible to make the problem better and so we manage it as best we can to achieve the above aims.
Managing dysphagia • This could be through: • Thickened fluids • Modified diets / alternative feeding • Positioning • Rate of feeding • Bolus size • Special equipment • Mouthcare • Suggesting changes to medication • Assistance to eat and drink • Supervision • Adjusting help according to changes in the person’s condition • Monitoring
The way that Speech and Language Therapists (SLTs) and other professionals describe dysphagia diets and thickened drinks is changing across the UK and the world.
Thickened fluids • Thin fluids • Slightly thick fluids • Mildly thick fluids • Moderately thick • Extremely thick
How to thicken drinks • Add the recommended number of flat scoops of • Resource Thicken Up Clear™ to a dry empty cup/glass • No. of level scoops: mildly= 2 moderately=4 extremely=8 • per 200mls • 2. Pour in 200mls of your chosen drink • 3. Immediately stir briskly with a spoon • until the powder is dissolved • 4. Leave to stand for 2 minutes until the drink has thickened • 5. Check consistency is correct - if it is not right you will have to pour the drink • away and start again
Top tips for thickening drinks • The drink should be thickened by staff before it is given to the patient or left on their table – to avoid aspiration if it is drunk unthickened • All liquids should be thickened (unless specified in SLT recommendations) – ie. all cold and hot drinks, fizzy drinks, soups, nutritional supplement drinks, gravy, alcoholic drinks etc • Be positive about the drink if you are preparing it for someone • Some people find cold thickened drinks more enjoyable, or drinks with • a stronger flavour, eg. squash rather than water • If the patient has any liquid or soluble medications, discuss with the • pharmacist and make your SLT aware. • NB. DO NOT leave the tub of thickener within reach of the patient, • as this is a choking risk if ingested accidentally •
Cups, spouts and straws • Spouts don’t let you control how fast the drink comes into your mouth • Wide spouts are particularly difficult • Spouts also encourage you to tip your head back, which is a bigger risk for the fluid going down too fast and into the airway • Straws are helpful for some people, but others find them hard to control • Straws can direct the drink towards the back of the mouth and it might go down into the throat too quickly • If possible, normal cups are often best for swallowing, because your head comes forwards and your lips can control the flow of drink • Other options include: • Nosey beakers, dysphagia cups • Controlled bolus cups • Steady hands cups
The importance of mouthcare • Why is good oral hygiene so important in the care of patients with dysphagia? • They are more likely to get food residue in the mouth • Eating and drinking may already be less enjoyable – without a clean mouth even more so • Poor oral hygiene means more bacteria in the mouth • Any food, fluid or saliva which is aspirated will transport those bacteria into the airway and the lungs • This greatly increases their chance of developing aspiration pneumonia
Mouth care guidance for care homes - NICE • NICE has some good clear guidance for care homes about mouth care and how to improve oral hygiene • https://www.nice.org.uk/about/nice-communities/social-care/quick-guides/improving-oral-health-for-adults-in-care-homes • This is a good booklet: • https://www.nice.org.uk/Media/Default/Oral_health_quick_guide/Oral_health_a_quick_guide_for_care_home_managers.pdf
Thank you for listening and participating today, we hope it has been helpful.Any questions?