Download
1 / 27
370 likes | 1.47k Views
Central Cord Syndrome. ?. Controversies in Management. =. Central cord syndrome typically presents in an elderly patient with pre-existing cervical spondylosis.

E N D
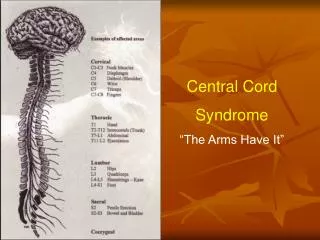
Central Cord Syndrome ? Controversies in Management =
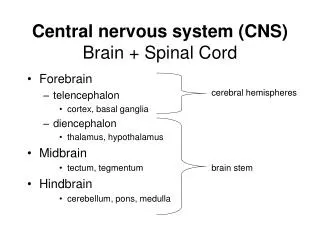
Central cord syndrome typically presents in an elderly patient with pre-existing cervical spondylosis. • The mechanism of injury involves hyperextension with pinching of the spinal cord between a thickened ligamentum flavum and a protruding anterior osteophyte or disc. • An associated fracture of a cervical vertebra is uncommon. Bruise on forehead is common. • The typical neurological deficit is symmetrical quadraparesis affecting the upper more than the lower limbs. Varying degrees of sensory loss
Epidemiology • 16.5% of spinal cord injuries in Australian series • Mean age 60 yrs, but huge variation amongst studies with inherent biases in patient population (ie children in some)
Associated Pathology • Disc protrusion was most common in younger patients • Followed by the subluxation, dislocation and fracture • Spondolytic bars, discs and ligamentum flavum hypertrophy were common in the older age group
Pathophysiology • Classically described, traumatic central hematomamyelia • Most medial fibres of CST within the lateral columns affected • No somatotopic organization has been shown • Alternative hypothesis suggests CST is more important for upper extremity, particularly finger dexterity
Outcome • Age is single biggest predictor of outcome • Patients over 70 show poorer ASIA scores at presentation and at discharge • Most patients under 50 are able to walk and have good bladder function • In one study on long term follow up mean = 8.9yrs), only 1/3 over 70 could walk independently and none regained bladder control
Outcome • In the upper limb, the distal roots were more severely affected than the proximal roots • 30% of younger patients had dexterity problems and 100% over 70 • Of those who died during study, they lived less than 20% of Life expectancy from the time of injury
Classic Paper • Schneider RC, Cherry G, Pantek H. The syndrome of acute central cervical spinal cord injury: with special reference to the mechanisms involved in hyperextension injuries of the cervical spine. J Neurosurg 1954;11:546-77
Classic Paper • Hyperextension of a degenerative cervical spine was the predominant mechanism of injury • Recovery followed a set pattern beginning with the lower limbs and ending with hand function • Authors stated that surgery was contraindicated
Controversies • Surgical vs. conservative management • Early vs. late surgery • Surgical approach
Controversies • Many advocate all patients be treated conservatively unless there is a major fracture or dislocation or extrinsic compression of the cord at presentation. • Some authors have suggested that surgery is indicated in selected cases, but none of these studies were prospective or randomized
Controversies • Surgical treatment has been shown to yield a longer period of discomfort from pain and weakness in certain cases. • Removal of offending lesions in the subacute period results in significant motor and sensory improvement in short-term and long-term follow-up. Chen et al
Chen et Al • Surgery was performed on average 10 days after trauma, 3 month follow up • Indications: failure of motor improvement, less than grade 3 power at 2 weeks with compression of neural tissue on imaging • Reported rapid resolution of hyperpathia with surgery and improved motor function
Controversies • Chen suggests that aggressive early decompression in selected patients, especially younger patients, improves outcome [retrospective review] • In studies of patients treated by medical therapy alone, younger patients faired better anyway [natural history]
Scientific Rationale for Surgery(Chen) • Edema in white matter of lateral columns in acute stage, without myelin change • Resulting from mechanical tear and possible secondary ischemia following compression • Hence, early removal of offending lesions may contribute to improve outcomes, especially before chronic myelopathy is demonstrated
Scientific Rationale for SurgeryFehlings & Tator • Experimental evidence shows that persistent compression of the spinal cord is a potentially reversible form of secondary injury • Severity of the pathological changes and the degree of recovery are directly related to the duration of acute compression • Experimental studies: neurological recovery is enhanced by early decompressive surgery
Controversial Case • 62 yo male • OPLL • Minor trauma • Central Cord Syndrome • Gr II in U/E • Gr IV in L/E • Methylprednisolone • Steady improvement for two weeks then reached plateau
Tator’s Opinion • Significant space occupying lesion must be removed • Although most patients still have a significant neurological deficit postoperatively especially in the small muscles of the hand • Prefers early as possible intervention, but admits data lacking to prove this point • Recommended laminectomy of C3 to C6 • Would supplement with lateral mass screws and plates if evidence of instability was found
H Nakagawa’s Opinion • Notes no evidence of fracture or dislocation • Given steady improvement over two weeks would not to rush into surgery • However would intervene at Plateau • Chose expansive laminoplasty • Tator notes controversy • Would supplement with lateral mass fixation if instability demonstrated
TJ Pentelenyi • Absolute indication for emergency surgery • Chose anterior approach for anterior pathology HC Park • Notes controversy and treatment • Treatment of choice conservative management skeletal traction and methylprednisolone in most cases • Surgical treatment to prevent future injuries • Anterior approach is dangerous
More Controversy • There are clinical studies to show that early decompressive surgery is best • Studies also showed no difference between early and late decompression • Some studies demonstrated no difference in surgical vs. nonoperative management
Conclusion • In cases of central cord syndrome with an obvious offending lesion, fracture or dislocation the treatment is less controversial • In cases where differences of opinion exist with no evidence to support, a prospective randomized controlled trial is required to determine optimal therapy