Download
1 / 12
120 likes | 134 Views
Explore the impact of a collaborative approach in care transitions, addressing high re-admission rates by improving processes and communication within healthcare teams. Realize the benefits of streamlining reports and enhancing patient care coordination.

E N D
Transitions of Care A Team Based ApproachCare Transformation Collaborative of R.I. Donna Soares RN, CDE, CDOE, CVDOE Nurse care manager University Family Medicine
Definition of Transitions of Care • Patient movement from one facility to another • Hospital to home, SNF to home, Hospital to rehab etc.
Currently in Rhode Island • Realization of high re-admission rates in our state • Many missing pieces in TOC process • eg. Don’t always receive reports from hospitals re: patient updates etc.
Before we Started • Where do we begin? • What do we want to accomplish? • Assess entire process – admission, pre-discharge, discharge, accessing medical records • Assess current internal TOC process flow, then turn to external areas
What We Did: • Analyzed existing TOC process via process mapping sessions • Involved entire team in workflow development and implementation • Made NCM aware of all inpatient admissions • Attempt to streamline TOC reports from multiple payers and CurrentCare (Direct Alerts)
What We Did: • Review payer reports – not always reliable • Fine tuned entire process through messaging in the EHR • Analyzed communication process amongst team (Secretaries and Medical Assistants) for TOC • Identified and implemented opportunities via process mapping
Things to Consider • Patient discharge needs • Available resources • Health care resources • Community resources • Continuity of care needs • Behavioral health • All these are handled by hospital d/c planner prior to hospital d/c.
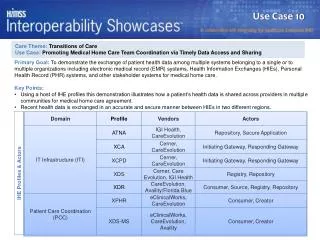
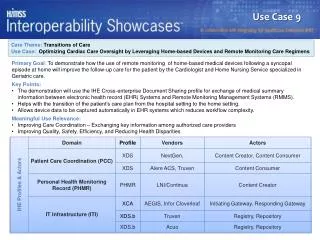
Patient Example • 41 y/o male with muscular dystrophy fell at home on 3/24/2015. Went to KCMH ER. DX – distal clavicle fracture. • 83 y/o grandmother is patient’s caretaker. She called our office on 3/25/2015 to schedule follow-up for him here. She was given an appointment for him for 3/30/2015. • With our process, I was notified of the upcoming appointment before I had notification of ER visit. I contacted patient’s grandmother and was able to facilitate an appointment with orthopedic for 3/27/2015.
Results: • NCM is not a solo sport • Team involvement is key with the TOC process • PCP needs to be coordinator for TOC • Developed at a glance identification of high risk patients in EHR • Eliminated much of paper trail
Results: • Dynamic and fluid process • Smoother TOC for our patients • Efficiencies gained with workflow redesign • Re-evaluate our re-admission rates
Moving Forward • Seamless TOC for the patient, for practice staff • Improved communication with all players in the state • Foster partnerships with hospital discharge planning staff and NCM • Involve specialists • Ongoing meetings with Healthcentric Advisors – involving representation from all healthcare arenas (hospitals, SNF’s, home care) • Improved data from payors (timely and actionable) • Triple Aim • lower healthcare costs, • improved satisfaction / experience of care, • improved care across the population)
Questions? Thank you! Resources: http://www.dea.ri.gov/Pocket%20Manual/2014%20Pocket%20Manual-November%205,%202014.pdf http://www.pcpci.org/ http://www.safetynetmedicalhome.org