Download
1 / 36
360 likes | 372 Views
This article explores the potential health effects of the military use of depleted uranium (DU), including its radioactive and chemo-toxic nature. It discusses the evidence for these health effects and provides information on the properties and usage of DU in military applications.

E N D
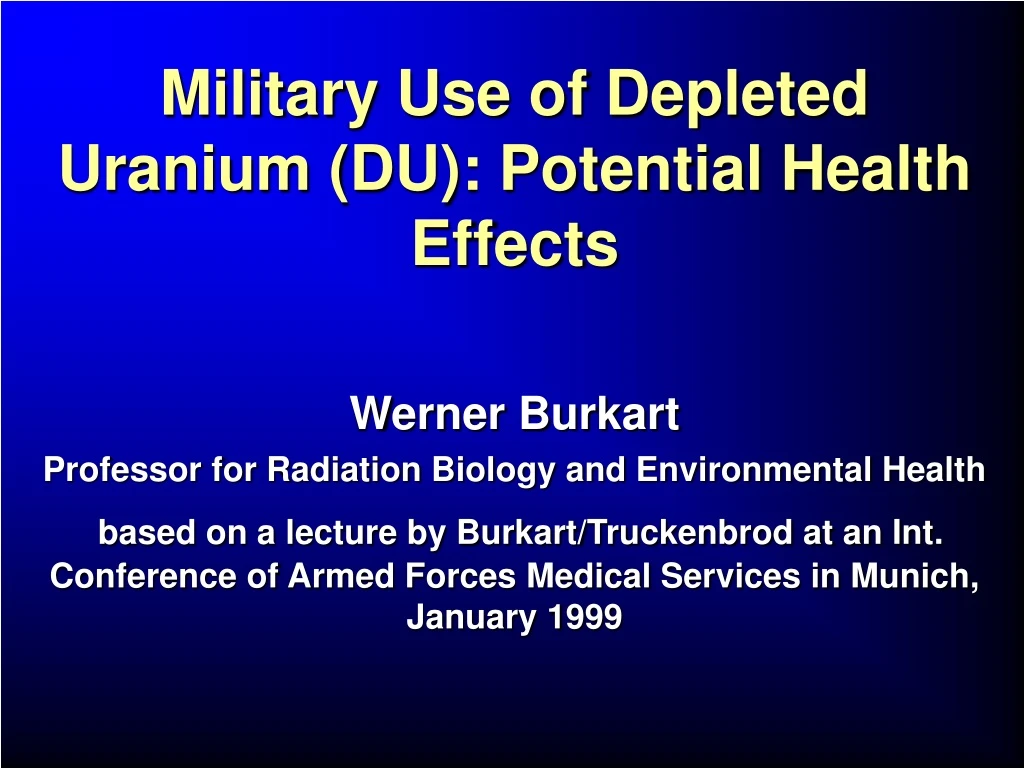
Military Use of Depleted Uranium (DU): Potential Health Effects Werner Burkart Professor for Radiation Biology and Environmental Health based on a lecture by Burkart/Truckenbrod at an Int. Conference of Armed Forces Medical Services in Munich, January 1999
Use of Depleted Uranium (DU) in ammunition • Gulf war: ~ 320 t • Kosovo conflict: ~ 10 t • Sarajevo safety zone: ~ 3 t DU is radioactive and chemo toxic • As a result of its use is there a risk of health effects? • Is there any evidence for these health effects ? Werner Burkart
DU-Use in Kosovo (X Major Targets)Approx. 31,000 rounds or 9 tons in more than 100 missions Werner Burkart
Uranium in the Earth Crust: 0.3 – 3.0 g/t Natural Uranium consists of three radioactive isotopes U-235 and U-238 are the origin of two different decay chains U-234 is a product of the decay chain of U-238 Werner Burkart
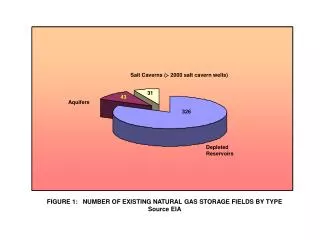
Feed, Product und Waste in aProcess for Uranium Enrichment Feed Unat (0.71% U-235) UF6 Waste: Depleted Uranium (DU) as Depleted UF6(0.3% U-235) Enrichment Process Enriched UF6 (3.6% U-235) Example: Pressurized Water Reactor Werner Burkart
DU is a waste product of uranium enrichment • Presently there are 570.000 t of DU stocked in the USA • The stockage of DU in steel containers is expensive • DU is cheap and available in large quantities Werner Burkart
Definition and Properties of Depleted Uranium (DU) • Content of U-235: 0.2 – 0.3 % • Low radioactivity • Practically pure -emitter and -radiation field through daughter productsHeavy metal with high density: 18.9 g/cm3 • chemotoxic as most heavy metals • pyrophoric Werner Burkart
Comparison between the Radiactivity of Unat and DU The activity of DU is 60% of that of Unat Werner Burkart
Decay Chain of U-238 • DU contains 99.8 % U-238 • U-238 is not in radioactive equilibrium with its daughter radionuclides • After few months equilibrium is reached between U-238, Th-234, Pa-234m Werner Burkart
Civilian Use of DU • Colour Glazing (red and yellow) • Steel alloys • Catalysts • Counterweights in fly wheels, fork lift trucks, keel lines of ships • Ballast in aircrafts (the first 550 Boing 747) • Shield material for -radiation (better than lead) Problem: Spontaneous ignition during the machining of the metal Werner Burkart
Military Use of DU • Shielding in Tanks • Ammunition (first time in 1991, Gulf War, 320 t) • The high velocity of DU ammunition permits to penetrate the reinforced armoring of tanks • On hitting the target DU ignites, forming an aerosol of DU particles and/or larger fragments • Aerosol: the particle size and the quantity depends on the impact angle , velocity and burning temperature Alternative to DU = Tungsten Werner Burkart
Anti Tank DU Ammunition Werner Burkart
Anti Tank DU Ammunition Werner Burkart
Target Hit by DU Ammunition Werner Burkart
30 mm DU Rounds Found in Kosovo Werner Burkart
Chemistry Uranium is present in all crystal and mantel rocks in trace amounts. The average abundance is 2 – 3 mg/kg. Uranium in the environment is dominated by U (IV) and U (VI) oxides: Anoxic: U (IV) (UO2) insoluble, found in minerals (USiO4) Surface water, body fluids: typically U (VI) (UO3 divalent cation UO22+) Uranium used in penetrators and armor is in the zero oxidation state, which is thermodynamically unstable even at low temperatures. When exposed to the environment it will eventually oxidize (corrode). The oxidation liberates a large amount of heat. Werner Burkart
Uranium metabolism Caveat: For more soluble uranium compounds intake is limited by consideration of chemical toxicity WHO limits for uranium intake: Drinking water: 2μg/L Tolerable Daily Intake (TDI) 0.6μg/kg body weight Adsorption in the gut for dietary (monomeric) forms: 2 – 5 % even less for particulate and insoluble forms Most affected tissues: kidney; U binds to proteins (acute effects) bone surface (radiation dose) liver red bone marrow No enrichment in thyroid gland Werner Burkart
Inhalation of different forms of uranium • Soluble forms cleared rapidly • Exotic (fired, “ceramic”?) forms may remain in lung, • tracheobronchial lymph nodes for years (Fisher 1988) • Hot particles → New CRP Werner Burkart
Aerosol characteristics A considerable fraction of the DU ammunition can become Aerosols Typical composition of an aerosol after hitting a solid target ca. 61 % U3O8 Type S ca. 18 % UO2 Type S ca. 20 % amorphous oxides Type F (Scripsick et al. 1984) 50 – 96 % of the aerosols can enter the lung AMAD < 10 m AMAD = Activity Median Aerodynamic Diameter Werner Burkart
Contamination of Sites • Dust/fine dust: loose contamination inside and outside military objects • Fragments in soilcorroded DU is soluble Remediation: elimination of the fragments, clean-up of the contaminated zones Potential Radiation Dose rates External:-Radiation, Th-234, Pa-234m Direct skin contact: 2mSv/h -radiation in tanks: 0.1 – 1.3 Sv/h Internal:-Radiation (U-238), and Werner Burkart
Possible ways of incorporation • Inhalation of dust particles of different size and solubility • Ingestion through food, water, swallowing of dust • Wound contamination • For military combat: shrapnel remaining in the body Werner Burkart
Uranium Metabolism The uranium compounds can be classified according to their solubility and consequent transportability from the respiratory organs into the body liquids (ICRP 66) Very slightly soluble ( S: low): UO2, U3O8 Moderately soluble (M: medium): UF4, UO3, UO4 Easily soluble (F: fast): UF6, UO2(NO3)2, UO2F2, UO2SO4 Uptake by the gastro-intestinal tract: f1 = 0.002: 0.2 % -”- (Moderately and very slightly soluble) f2 = 0.02: 2.0 % will transfer to blood (soluble) Werner Burkart
Health consequences of the incorporation of DU Werner Burkart
The lung as target organ • The lung is the primary organ at risk from inhalation of Type S uranium compounds • The biological half-life of these compounds in the alveolar region of the lungs can be as long as 16 years • Complete retention by lymph nods is assumed • Particles in the upper region of the respiratory system move by mucociliary transport to the gastro-intestinal tract • 0.2 % is reabsorbed by the intestine and the rest is eliminated via feces Werner Burkart
Kidney and bone as critical target organs for soluble uranium components • Inhaled uranium (Type F) will rapidly transfer to blood • 98 % of ingested uranium (F) will be eliminated through the feces and 2% absorbed by the intestine For both types of uptake • U as a heavy metal, is chemotoxic for the kidney (limit: 3 gU/g of kidney tissue, 0.9 mg/both kidneys) • Bone is considered critical for accumulated radiation dose Werner Burkart
Model Predictions of the Uranium Content of Bone as a Function of Time after Injection into Blood for Different Ages Werner Burkart
Annual limits for U-238 (StrlSchV, 1989) Werner Burkart
Results of Animal Studies (dogs) The Solubility of the inhaled uranium compounds determines the target organ Werner Burkart
Typical values Werner Burkart
Analytical Methods(detection limits) Werner Burkart
Studies on 33 Gulf-War veterans • Cohort of US Soldiers wounded by DU or present in a vehicle hit by DU ammunition (friendly fire) • The study started 3 years after the war • Blood parameters: no significant alteration • Uranium in urine DU fragments in the body release uranium which shows up in urine (increased mobility of uranium with time) Werner Burkart
Available Epidemiological Information • There are no studies on populations exposed only to uranium • Uranium is only a minor contributor to naturally or artificially elevated radiation exposures • Indirect Risk Evaluation • Experimental radiobiological information • Mechanistic considerations Werner Burkart
Tiredness 20.5% Skin rash 18.4% Headache 18.0% Muscle and joint 16.8% pain Loss of memory 14.0% and other symptoms Shortage of breath 7.9% Sleeping problems 5.9 % Diarrhea and other 4.6% disturbances of the gastro-intestinal tract Other symptoms 3.6% Chest pain 3.5% With no problems 12.3% In Search of a Definition of the Gulf War Syndrome I The 10 most frequently reported problems by Gulf War veterans (N = 52.835) A Guide to Gulf War Veterans Health, 1998 Continuing Medical Education Program Werner Burkart
No diagnosis 26.5% Musculosceletal and 25.2% Connective tissues Disturbance of the 15.1% Psychological equilibrium Respiratory system 14.3% Skin tissues 13.5% Digestive system 11.4% Nervous system 8.3% Circulatory system 7.1% Infectious diseases 7.0% Injuries and poisoning 4.7% Urogenital system 3.4% Neoplasm 0.4% In Search of a Definition of the Gulf War Syndrome II Distribution of diagnoses (N = 52.835 veterans) A Guide to Gulf War Veterans Health, 1998 Continuing Medical Education Program Werner Burkart
Other Agents Discussed in Connection with the Gulf War Syndrome • Fire fumes, soot, various harmful chemicals • Napalm • Several toxins • Vaccines • Pesticides • Insecticides • Protective substances against chemical weapons Werner Burkart
Summary • No acute risk • Theoretical cancer risk due to DU contamination much smaller than that from natural radiation • Complications due to perception (emotional, psychological, stress-related) • Possible future actions: • Radio-ecological assessment, dose estimates • Health-effects assessment • Occupational hygiene: monitoring before/after deployment, documentation of DU activities, doses, health statistics Werner Burkart