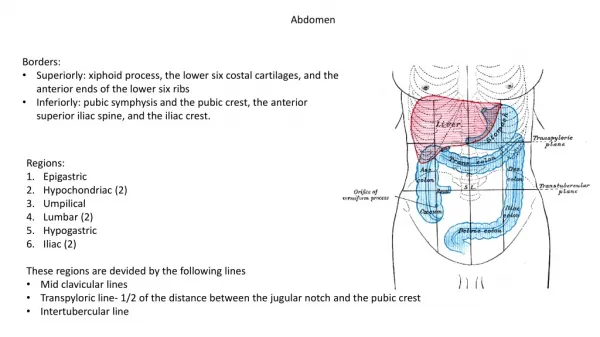
Download

1 / 132
1.32k likes | 1.33k Views
Learn about the imaging characteristics and treatment options for carcinoid and colorectal cancer, two types of gastrointestinal cancers that can cause abdominal pain, bleeding, and bowel obstruction. Discover how CT and MRI scans can aid in diagnosis and staging, and explore the benefits of surgery, chemotherapy, and radiation therapy in treating these cancers.

E N D
ABDOMEN Gastrointestinal
Gastrointestinal: • Carcinoid • Colorectal Cancer • Crohn Disease • Free Intraperitoneal Air • Gastric Carcinoma • Intussusception • Ischemic Bowel • Large Bowel Obstruction • Mesenteric Adenitis • Mesenteric Ischemia • Small Bowel Obstruction • Volvulus
Description: • Carcinoids are rare, slow-growing cancers which start in the lining of the gastrointestinal tract.
Etiology: • Unknown; however, genetic involvement is suspected.
Epidemiology: • Overall, 1.5 cases per 100,000 populations. They occur mostly in the appendix (50%) and small bowel (20%). The ileum is the most frequent site of involvement in the small bowel. Females and older adults are more commonly affected.
Signs and Symptoms: • The signs and symptoms may be vague. Patients may experience abdominal pain, bleeding, and bowel obstruction.
Imaging Characteristics: • Primary tumors may be small. Aggressive tumors >2 cm may have a necrotic center. May mimic a lymphoma. CT • Appear as a bright wall mass with IV contrast. • Thick fibrotic stranding radiates from the mass to adjacent bowel. • Usually metastasize to the liver, are hypervascular, and best seen on the arterial phase.
MRI • T1-weighted signal is isointense to muscle. • T1-weighted postgadolinium shows bright signal on delayed studies. • T2-weighted signal may vary from isointense to hyperintense to muscle.
Treatment: • Surgery is the treatment of choice. Chemotherapy is helpful for metastatic spread.
Prognosis: • Results are better if complete resection of the localized tumor is accomplished.
Figure 1. Carcinoid B A Pre- (A) and postcontrast (B) CTs of the abdomen show an enhancing, partially calcified, stellate mid-abdominal mesenteric mass with radiating bands of fibrosis and retraction of the surrounding small bowel, giving a classic "sunburst" appearance.
Figure 2. Carcinoid Contrast-enhanced CT (CECT) coronal multiplanar reconstruction (MPR) image shows similar findings as the axial images. In this image, multiple low-attenuation liver metastases can be seen.
Description: • Colorectal cancer (adenocarcinoma of the colon) is the most common malignant tumor affecting the gastrointestinal tract. Colorectal cancer often begins as a polyp which may become malignant if left untreated.
Etiology: • A number of factors such as heredity, inflammatory bowel disease (eg, ulcerative colitis and Crohn disease), physical inactivity, overweight and obesity, diabetes, diet, smoking, and alcohol intake are thought to play a role in the development of colorectal cancer.
Epidemiology: • Colorectal cancer is the third leading cause of cancer death for men and women in the United States. African Americans have a higher incidence rate than white people, while Hispanics/Latinos, American Indians, and Alaska natives have a lower incidence rate. Male are slightly more affected than females. Incidence and death rates increase in individuals 50 years and older.
Signs and Symptoms: • In its early stage, colorectal cancer is often asymptomatic. Patients may experience rectal bleeding, blood in the stool, cramping lower abdominal pain, change in bowel habits, and new onset of constipation.
Imaging Characteristics: • Primary tumor may be a colon polyp usually >1 cm. Polyps may appear as sessile or pedunculated mass arising from the bowel wall and protruding into the lumen.
CT • Chest, abdomen, and pelvic scan for staging purposes. • Central low attenuation represents hemorrhage or necrosis. • Air within the tumor may indicate ulceration. • Regional lymph nodes >1 cm are considered positive for metastatic spread. • Distant metastatic spread is mostly seen in the liver (75%), lung (5% to 50%), adrenal gland (14%), and elsewhere. • Thin-section imaging is required for CT colonography. • Fecal and fluid tagging is beneficial in CT colonography.
MRI • Normal colon has a thin wall with haustrations, and enhances minimally with IV contrast. • T2-weighted single-shot echo-train spin-echo and True-FISP help control for bowel motion. • IV contrast-enhanced with fat suppression T1-weighted-spoiled gradient or 3D gradient echo is helpful in evaluating the colon. • Dark-lumen technique may show a polyp protruding into the lumen. • Endorectal MR may be helpful in evaluating the rectum.
Treatment: • Depending on the stage of the cancer, surgery, chemotherapy, and radiation therapy may be used.
Prognosis: • Colon screening is beneficial in early detection and treatment. The 5-year survival for colorectal cancer (including all stages) is about 65%.
Figure 1. Colorectal Cancer CECT shows abnormal mural thickening of the mid transverse colon with luminal narrowing and surrounding soft tissue bands extending into the surrounding fat which likely represents extracolonic tumor extension.
Figure 2. Colorectal Cancer CECT with positive oral contrast shows abnormal mural thickening of the right hemicolon.
Figure 3. Colorectal Cancer CECT coronal MPR image shows a several centimeter segment of thickened bowel wall involving the mid-right colon. This is typical of colon cancer.
Description: • Crohn disease is an inflammatory condition which can affect any part of the alimentary tract. However, the small bowel, specifically the terminal ileum, is most commonly affected.
Etiology: • Though the precise cause remains unknown, there seems to be a combination of genetic, immunologic, and infectious factors involved.
Epidemiology: • Crohn disease can occur at any age; however, the disease usually presents in adolescents and young adults between the ages of 15 and 35 years. It has a bimodal distribution with the first peak being in the teens and twenties and the second peak occurring in the fifties through the seventies.
Signs and Symptoms: • Patients present with persistent or recurrent diarrhea, abdominal pain with cramps, weight loss, and fever.
Imaging Characteristics: • Key characteristics include: (1) bowel wall thickening greater than 1 cm; (2) involvement of >15 cm bowel; and (3) mural enhancement. CT • IV contrast shows marked bowel wall enhancement. • Fistula may be seen. • Mesenteric inflammation is seen as diffuse haziness and increased density in the mesenteric fat. • Normal bowel "skip areas" may be seen between diseased segments of bowel.
MRI • T2-weighted single-shot echo-train spin-echo and IV gadolinium-enhanced T1-weighted with fat suppression spoiled gradient echo demonstrates dilated bowel and inflammatory changes. • 3D gradient echo demonstrates characteristics findings: mural enhancement, skip lesions (patchy areas of inflammation), and mesenteric inflammatory changes.
Treatment: • Is focused on reducing the inflammation and maintaining good nutrition.
Prognosis: • There is no cure for this disease. Patients with Crohn disease are at an increased risk for colorectal cancer.
Figure 1. Crohn Disease CECT axial images (A,B) show intense enhancement of the mucosa and low-attenuation edematous thickened submucosa of the terminal ileum consistent with Crohn disease.
Figure 2. Crohn Disease CECT coronal MPR image in the same patient shows mesenteric hypervascularity ("comb sign") and proliferation of the adjacent mesenteric fat.
Figure 3. Crohn Disease Postcontrast T1W fat saturation MR image (e-THRIVE) shows an enhancing thickened long segment terminal ileum (arrow) as well as "comb sign" with mesenteric hypervascularity (arrowhead).
Description: • Free air in the peritoneal cavity, also known as a pneumoperitoneum, is a collection of air or gas in the peritoneal cavity.
Etiology: • This condition can be the result of several factors such as: iatrogenic perforation (eg, laparoscopy, leaking surgical anastomosis, enema tip), disease process (eg, ulcer, ingested foreign body, ruptured intestine), and penetrating trauma. The most common cause is perforated ulcer.
Epidemiology: • It may occur in anyone who has experienced any of the above-listed factors.
Signs and Symptoms: • Pain and tenderness usually result from a perforation of the bowel.
Imaging Characteristics: • Best detected on lung windows (WL = -400 to -600; WW = 1000 to 2000). CT • Gold standard for detection of a pneumoperitoneium. • IV contrast may not be required. • Oral contrast (water soluble) may be used to better visualize the GI tract and to demonstrate a leak in the bowel. • Appears hypodense. • Free air is classified according to the anatomical location. • Scanning in the decubitus position will assist in interpreting difficult cases.
Treatment: • Depends on the etiology.
Prognosis: • Depends on the etiology.
Figure 1. Free Intraperitoneal Air Axial CT shows a large amount of intra-abdominal free air outlining multiple loops of bowel.
Figure 2. Free Intraperitoneal Air Axial CT demonstrating less dramatic example of extraluminal intraabdominal free air (arrows) in a patient with a duodenal perforation.
Description: • Gastric (adenocarcinoma) carcinoma is one of the most common cancers in the world. Adenocarcinomas make up approximately 95% of all malignant cancers affecting the stomach.