Download
1 / 1
10 likes | 112 Views
TuPe2.3C18 3 rd IAS Conference Rio de Janeiro 24-27 July 2005 Joel E. Gallant, MD, MPH 1830 E. Monument St, Room 443 Baltimore, MD 21287 E-mail: jgallant@jhmi.edu.

E N D
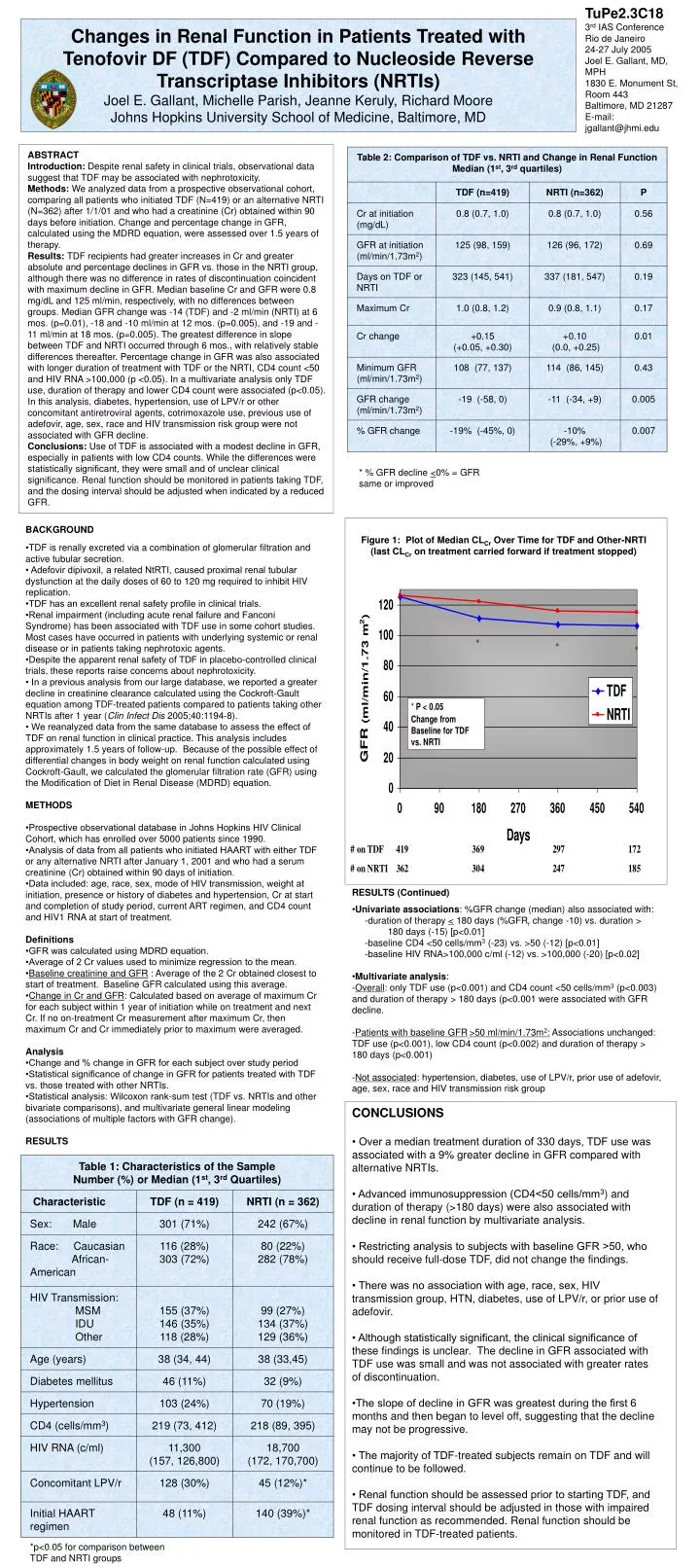
TuPe2.3C18 3rd IAS Conference Rio de Janeiro 24-27 July 2005 Joel E. Gallant, MD, MPH 1830 E. Monument St, Room 443 Baltimore, MD 21287 E-mail: jgallant@jhmi.edu Changes in Renal Function in Patients Treated with Tenofovir DF (TDF) Compared to Nucleoside Reverse Transcriptase Inhibitors (NRTIs) Joel E. Gallant, Michelle Parish, Jeanne Keruly, Richard Moore Johns Hopkins University School of Medicine, Baltimore, MD ABSTRACT Introduction: Despite renal safety in clinical trials, observational data suggest that TDF may be associated with nephrotoxicity. Methods: We analyzed data from a prospective observational cohort, comparing all patients who initiated TDF (N=419) or an alternative NRTI (N=362) after 1/1/01 and who had a creatinine (Cr) obtained within 90 days before initiation. Change and percentage change in GFR, calculated using the MDRD equation, were assessed over 1.5 years of therapy. Results: TDF recipients had greater increases in Cr and greater absolute and percentage declines in GFR vs. those in the NRTI group, although there was no difference in rates of discontinuation coincident with maximum decline in GFR. Median baseline Cr and GFR were 0.8 mg/dL and 125 ml/min, respectively, with no differences between groups. Median GFR change was -14 (TDF) and -2 ml/min (NRTI) at 6 mos. (p=0.01), -18 and -10 ml/min at 12 mos. (p=0.005), and -19 and -11 ml/min at 18 mos. (p=0.005). The greatest difference in slope between TDF and NRTI occurred through 6 mos., with relatively stable differences thereafter. Percentage change in GFR was also associated with longer duration of treatment with TDF or the NRTI, CD4 count <50 and HIV RNA >100,000 (p <0.05). In a multivariate analysis only TDF use, duration of therapy and lower CD4 count were associated (p<0.05). In this analysis, diabetes, hypertension, use of LPV/r or other concomitant antiretroviral agents, cotrimoxazole use, previous use of adefovir, age, sex, race and HIV transmission risk group were not associated with GFR decline. Conclusions: Use of TDF is associated with a modest decline in GFR, especially in patients with low CD4 counts. While the differences were statistically significant, they were small and of unclear clinical significance. Renal function should be monitored in patients taking TDF, and the dosing interval should be adjusted when indicated by a reduced GFR. * % GFR decline <0% = GFRsame or improved BACKGROUND •TDF is renally excreted via a combination of glomerular filtration and active tubular secretion. • Adefovir dipivoxil, a related NtRTI, caused proximal renal tubular dysfunction at the daily doses of 60 to 120 mg required to inhibit HIV replication. •TDF has an excellent renal safety profile in clinical trials. •Renal impairment (including acute renal failure and Fanconi Syndrome) has been associated with TDF use in some cohort studies. Most cases have occurred in patients with underlying systemic or renal disease or in patients taking nephrotoxic agents. •Despite the apparent renal safety of TDF in placebo-controlled clinical trials, these reports raise concerns about nephrotoxicity. • In a previous analysis from our large database, we reported a greater decline in creatinine clearance calculated using the Cockroft-Gault equation among TDF-treated patients compared to patients taking other NRTIs after 1 year (Clin Infect Dis 2005;40:1194-8). • We reanalyzed data from the same database to assess the effect of TDF on renal function in clinical practice. This analysis includes approximately 1.5 years of follow-up. Because of the possible effect of differential changes in body weight on renal function calculated using Cockroft-Gault, we calculated the glomerular filtration rate (GFR) using the Modification of Diet in Renal Disease (MDRD) equation. METHODS •Prospective observational database in Johns Hopkins HIV Clinical Cohort, which has enrolled over 5000 patients since 1990. •Analysis of data from all patients who initiated HAART with either TDF or any alternative NRTI after January 1, 2001 and who had a serum creatinine (Cr) obtained within 90 days of initiation. •Data included: age, race, sex, mode of HIV transmission, weight at initiation, presence or history of diabetes and hypertension, Cr at start and completion of study period, current ART regimen, and CD4 count and HIV1 RNA at start of treatment. Definitions •GFR was calculated using MDRD equation. •Average of 2 Cr values used to minimize regression to the mean. •Baseline creatinine and GFR : Average of the 2 Cr obtained closest to start of treatment. Baseline GFR calculated using this average. •Change in Cr and GFR: Calculated based on average of maximum Cr for each subject within 1 year of initiation while on treatment and next Cr. If no on-treatment Cr measurement after maximum Cr, then maximum Cr and Cr immediately prior to maximum were averaged. Analysis •Change and % change in GFR for each subject over study period •Statistical significance of change in GFR for patients treated with TDF vs. those treated with other NRTIs. •Statistical analysis: Wilcoxon rank-sum test (TDF vs. NRTIs and other bivariate comparisons), and multivariate general linear modeling (associations of multiple factors with GFR change). RESULTS Figure 1: Plot of Median CLCr Over Time for TDF and Other-NRTI(last CLCr on treatment carried forward if treatment stopped) RESULTS (Continued) •Univariate associations: %GFR change (median) also associated with: -duration of therapy < 180 days (%GFRr change -10) vs. duration > 180 days (-15) [p<0.01] -baseline CD4 <50 cells/mm3 (-23) vs. >50 (-12) [p<0.01] -baseline HIV RNA>100,000 c/ml (-12) vs. >100,000 (-20) [p<0.02] •Multivariate analysis: -Overall: only TDF use (p<0.001) and CD4 count <50 cells/mm3 (p<0.003) and duration of therapy > 180 days (p<0.001 were associated with GFR decline. -Patients with baseline GFR>50 ml/min/1.73m2: Associations unchanged: TDF use (p<0.001), low CD4 count (p<0.002) and duration of therapy > 180 days (p<0.001) -Not associated: hypertension, diabetes, use of LPV/r, prior use of adefovir, age, sex, race and HIV transmission risk group CONCLUSIONS • Over a median treatment duration of 330 days, TDF use was associated with a 9% greater decline in GFR compared with alternative NRTIs. • Advanced immunosuppression (CD4<50 cells/mm3) and duration of therapy (>180 days) were also associated with decline in renal function by multivariate analysis. • Restricting analysis to subjects with baseline GFR >50, who should receive full-dose TDF, did not change the findings. • There was no association with age, race, sex, HIV transmission group, HTN, diabetes, use of LPV/r, or prior use of adefovir. • Although statistically significant, the clinical significance of these findings is unclear. The decline in GFR associated with TDF use was small and was not associated with greater rates of discontinuation. •The slope of decline in GFR was greatest during the first 6 months and then began to level off, suggesting that the decline may not be progressive. • The majority of TDF-treated subjects remain on TDF and will continue to be followed. • Renal function should be assessed prior to starting TDF, and TDF dosing interval should be adjusted in those with impaired renal function as recommended. Renal function should be monitored in TDF-treated patients. *p<0.05 for comparison between TDF and NRTI groups






















