Download
1 / 11
110 likes | 178 Views
Review of the Last Lecture. began our discussion of information asymmetry in the healthcare market Two aspects to the information asymmetry i) HC providers more knowledgeable about HC ii) HC providers more knowledgeable about HC => HS

E N D
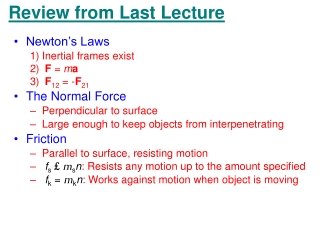
Review of the Last Lecture • began our discussion of information asymmetry in the healthcare market • Two aspects to the information asymmetry • i) HC providers more knowledgeable about HC • ii) HC providers more knowledgeable about HC => HS • Since the patient’s demand for HC is a derived demand (from demand for HS) HC provider can control the position of the demand curve => makes the demand curve endogenous • information asymmetry leads to market failure unless the healthcare provider is a perfect agent • continue with this discussion today
Policy Response to Information Asymmetry in the HC Market • Information asymmetry introduces a conflict of interest for the HC provider self interest (income) • patient’s interest • Policy response to info asymmetry certification by professional associations assures quality and provides assurance higher price reflects higher quality. • Also avoid exploitation (professional ethics/discipline) /// • by definition supplier-informed demand is the goal of the agency role
Consequence of Certification HC Providers • Certification (credentialing) of HC providers confers control over entry into the profession and over the behavior of the profession’s members. • Certification creates scope for exercising monopoly power by the professional organization that controls certification (restrict entry and limit competition among members) • Thus, certification to address market failure from information asymmetry may introduce another source of market failure => monopoly power
HC Provider as Perfect Agent • Information Asymmetry not a problem if provider is a perfect agent • Perfect agent chooses for the patient what the patient would have chosen for him or herself if the patient had had the same medical knowledge as the provider demand curve is where it should be • however, unlikely HC provider is a perfect agent • in real world agency relationship is incomplete • Demand curve can be shifted by HC provider advice; i.e. demand is endogenous normative and positive implications to be discussed later when we look at the theory of the practitioner firm ///
Evidence in Support of SID • price controls on physicians have often led to increased utilization per patient (boost income by increasing utilization if P fixed) • substantial variation in HC utilization across regions with similar populations but different DOC/POP ratios is often attributed to SID • empirical evidence that clinical decisions for a patient influenced by financial incentives for the doctor, e.g., • 1. Salaried GPs provide less care per patient than fee-for-service GPs • 2. HMOs have lower hospitalization rates than fee-for-service patients • 3. Monitoring, e.g. in Sask, in 1974 hysterectomy rate by 1/3 when Drs, but not patients, informed that the procedure would be monitored. ///
Counter Argument to SID • if Drs. can induce demand, how come they don’t own the world? • i.e. if physician behaviour isn’t constrained by autonomous consumer demand what does limit the P they can charge for a given Q, or the volume of services demanded at a given P (Diagram)? => will look at some possible answers when we look at theories of the practitioner firm ///
Alternative Explanations for the Link between Supply and Demand • Doc/Pop ratio (i.e.increased supply) less travel time and waiting time to see Dr. own time price demand shifts to the right, i.e., demand more HC at each price for HC since overall cost . • as Doc/Pop Dr. takes more time with each patient perceived quality of care WTP shifts demand to the right • End of our discussion of info asymmetry and market failure in the HC sector.///
Evaluating Healthcare Programs: Section VI of the Course outline • Will look at three methods of analyzing healthcare programs • - cost-benefit analysis • - cost-effectiveness analysis • - cost-utility analysis • discuss - how to conduct each type of analysis • - issues that need to be addressed in conducting the analysis • - strengths and weaknesses of each method of analysis ///
Cost-Benefit Analysis: CBA • CBA is a method for assessing the economic viability of a project. • A project generates a flow of: annual costs: C1, C2, C3, …,CT • annual benefits: B1, B2, B3, …,BT • the C’s and B’s must be expressed in dollars • in CBA these flows are expressed as present values of the costs and of the benefits => need a discount rate r • r is the rate at which we discount a dollar to be received(spent) one year from now, e.g., if r = 0.05 a dollar one year from now is worth 1/(1.05) = $0.952 today, a dollar two years from now is worth 1/(1.05)2 = $0.907, etc. • in general, the present value of a dollar of costs(benefits) incurred(received) n years from now is 1/(1+ r)n
The Present Value of the Benefits and of the Costs, and the NPV • compute the present value of the benefits (in $s): • PVB = B1/(1+r) + B2/(1+r)2 +…+ BT/(1+r)T • = t Bt/(1+r)t t = 1, …, T • compute the present value of the costs (in $s): • PVC = C1/(1+r) + C2/(1+r)2 +…+ CT/(1+r)T • = t Ct/(1+r)t t = 1, …, T • compute the net present value NPV = PVB – PVC ///
The Net Present Value Criterion • if NPV > 0 project is economically feasible • if NPV = 0 indifferent • if NPV < 0 project is not economically feasible • if funds are limitless implement all projects that are economically feasible • if funds are limited implement the set of projects that maximizes NPV for the available funds. ///