Download
1 / 21
220 likes | 262 Views
Learn about oral ulceration, including types like Recurrent Aphthous Stomatitis and Recurrent Oral Ulceration, associated diseases, and management strategies. Oral ulcers can be recurrent, single episodes, or secondary to systemic conditions.

E N D
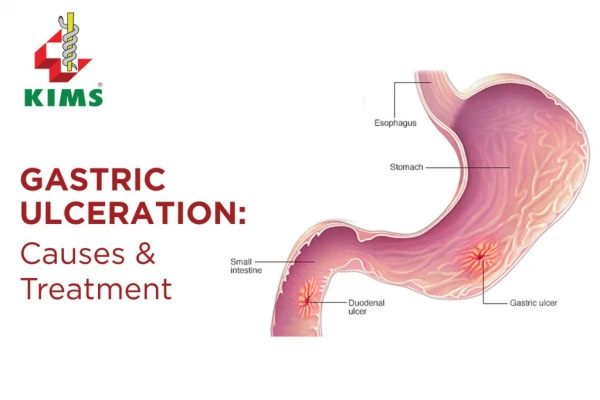
Definition – what is an ulcer? • Full thickness breach of the mucosal epithelium • Exposes nerve endings underlying the lamina propria • Typical symptoms – pain, soreness, discomfort when eating spicy, acidic foods • Can be superficial or extend into tissues underlying the surface epithelium – to submucosa, muscle or periosteum
Classification • Recurrent Apthous Stomatitis (RAS) • Recurrent Oral Ulceration (ROS) – occurring secondary to known or unknown systemic disease/infection • Single episodes of ulceration – trauma, burns, iatrogenic, Squamous Cell Carcinoma • See Table 1 for basic classification overview
Recurrent Apthous Stomatitis (RAS) • Defines recurring episodes of ulceration in healthy individuals • 20% prevalence • Occurring more commonly up to 30yrs but can persist >30yrs • 3 sub-types: Minor, Major or Herpetiform – depending on keratanised/non-keratanised surface and healing characteristics • Features vary with sub-type
Recurrent Oral Ulceration (ROU) • Patients with systemic disease may present with ROU • The aetiology and pathogenesis is directly linked to the underlying disorder • Examples: • Crohn’s Disease • Behcet’s Syndrome • Orofacial Granulomatosis • Leukaemia
Pathogenesis of RAS • Genetic predisposition – positive family history in approx. 1/3 patients • Immunological Factors – T Helper cells & Natural Killer cells predominate in early lesions followed by cytotoxic cells & antibody dependant cellular cytotoxicity
Aetiology - RAS • Genetic predisposition • Immune Deficiency • Hormonal link – fall in progesterone levels during menstrual cycle • Mucosal Integrity • Nutritional/Haematinic Deficiencies – e.g. iron, folate, vitamin B12 • Stress
Features of RAS Minor • Approx 80% of RAS cases • 10-40yrs • Ovoid/round ulcers • <10 mm in diameter • Yellow with red halo • Non-keratinised mucosa e.g. lips, cheek, floor of mouth • Groups of 1-6 ulcers • Heal in <14 days • No scarring
Major • 10% of RAS cases • >10mm • Crops of 2-5 ulcers • Keratinised and non-keratinised mucosa • Heal with scarring • Longer duration – can last several weeks (10-40 days) • More painful than minor • Frequent recurrence
Herpetiform • Common in older groups & females • Recurrent crops of small ulcers – multiple pinhead ulcers (which may look “herpetic”) – 0.5-3mm • Can increase in size to leave large ragged ulcers • Any oral site • Heal without scarring up to 14 days • Extremely painful • Occur continuously
Aetiology - ROU • Pathogenesis directly linked to underlying medical disorder • Secondary to systemic or infectious disease • Haematological – Neutropenia, Leukaemia • Rheumatological – Reactive Arthritis • Gastrointestinal – Chrons disease, ulcerative colitis, OFG • Dermatological – Lichen Planus, Erythema multiforme • Viral – HIV, ANUG, Herpetic gingivostomatitis • Bacterial – Tuberculosis • Behcet’s Syndrome
Behcet’s Syndrome • Auto-inflammatory condition • Apthous like oro-genital ulceration and ocular disease – uveitis • More common in males in 3rd decade • Racial distribution – countries bordering the Mediterranean due to genetic predisposition – HLA tissue types associated HLA-B12, HLA-DR2 and HLA-B51 • Diagnosis based on following criteria – a patient should have one major and two minor of the following: Major Recurrent oral ulceration Recurrent genital ulceration Ocular disease Cutaneous disease Minor Sero-negative arthritis Gastrointestinal disease Vascular Complications Central nervous system involvement
Behcet’s contd… • Oral ulceration similar to RAS • More frequent episodes • More ulcers per crop • Soft palate and oropharynx more commonly involved • More pronounce scarring • Greater resistance to treatment
Reactive Arthritis (Reiter’s Syndrome) • Autoimmine condition • Inflammation of large joints • Inflammation of the eyes – conjunctivitis or uveitis • Urethritis • Mucocutaneous lesions • Patients may present with apthous type ulceration
Single episodes of ulceration • Trauma – burns - chemical, thermal • Iatrogenic • Non-accidental injury • Cessation of smoking may aggravate ulceration
Diagnosis • Based on history and clinical features • To exclude underlying systemic conditions diagnostic testing as follows is required: Full Blood count, Haematinics – ferritin, folate, vitamin B12 Serological test for coeliac disease - tissue transglutaminase antibody or antiendomysial antibody • Clinical Features: site,size, shape, number of ulcers in crop, frequency & duration of episodes, age of onset, any systemic features? • Tissue biopsy if SCC suspected
Management & Treatment First Line Therapies • Good OH • Dispersible Doxycycline (100mg) & CHX mouthwashes • Topical Analgesics – 0.15% Benzydamine Hydrochloride (Difflam) or 1% Lidocaine ointment • Mucosal protectants – carboxymethylcellulose (orobase) • Topical Corticosteroids (on prescription) – 2.5mg Hydrocortisone muco-adhesive buccal tablet, 0.5mg soluble betamethasone phosphate tablets (mouthwash) or BeclometasoneDipropionate Spray Fluticasone propionate spray, mouthwash or ointment (off prescription)
Second Line Therapies • Systemic corticosteroid/immunosuppressive treatment for severe cases • Azathioprine • Clofazimine • Colchicine *Only under consultant-led treatment*
Referral of Suspicious Lesions When to Refer?? • Single ulcers persisting for longer than 3 weeks • Ulcers with an indurated border • Ulceration unresponsive to topical therapy • ROU of uncertain aetiology • RAS impacting on an individuals quality of life • Suspected SCC – URGENT referral
References • ORAL ULCERATION: AN OVERVIEW OF DIAGNOSIS AND MANAGEMENT PRIYA THAKRAR, SHAHID I CHAUDHRY Prim Dent J. 2016;5(1):30-33 • Oral Medicine: 1. Ulcers: Aphthous and other Common Ulcers David H Felix, Jane Luker, Crispian Scully Dental Update 2012; 513-519