Download
1 / 22
300 likes | 792 Views
Physiology of High-Altitude. Chapter 43. Effects of Low Barometric Pressures on the Body. Barometric Pressures: at 10,000 feet , only 523 mm Hg; at 50,000 feet , 87 mm Hg. This decrease in barometric pressure is the basic cause

E N D
Physiology of High-Altitude Chapter 43
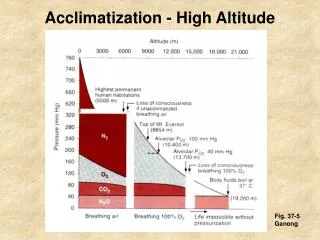
Effects of Low Barometric Pressures on the Body • Barometric Pressures: at 10,000 feet, only 523 mm Hg; at 50,000 feet, 87 mm Hg. • This decrease in barometric pressure is the basic cause • of all the hypoxia problems in high-altitude physiology because, as the barometric pressure decreases, the atmospheric oxygen partial pressure decreases • proportionately, remaining at all times slightly less than 21 per cent of the total barometric pressure—Po2 at sea level about 159 mm Hg, but at 50,000 feet only18 mm Hg.
At Mount Everest • Barometric pressure falls from the normal sea-level value of 760 mm Hg to 253 mm Hg, which is the usual measured value at the top of 29,028–foot Mount Everest. • Forty-seven millimeters of mercury of this must be water vapor, leaving only 206 mm Hg for all the other gases. • In the acclimatized person, 7 mm of the 206 mm Hg must be carbon dioxide, leaving only 199 mm Hg. One fifth of this 199 mm Hg would be oxygen and four fifths would be nitrogen; that is, the Po2in the alveoli would be 40 mm Hg. However, alveolar oxygen is continually being absorbed into the blood, leaving about 35 mm Hg oxygen pressure in the alveoli.
Acute Effects of Hypoxia • In the unacclimatizedperson breathing air, beginning at an altitude of about 12,000 feet are: • drowsiness, • lassitude, • decreased mental proficiency, which decreases judgment, memory, and performance of discrete motor movements. • mental and muscle fatigue, • headache, • nausea • twitchingsor seizures above 18,000 feet • coma above 23,000 feet, followed by death.
Acute Mountain Sickness • A small percentage of people who ascend rapidly to high altitudes become acutely sick and can die if not given oxygen or removed to a low altitude. • 1. Acute cerebral edema vasodilatation of cerebral blood vessels. 2. Acute pulmonary edema. • Allowing the person to breathe oxygen usually reverses the process within hours.
Acclimatization to Low PO2 • A person remaining at high altitudes for days, weeks, or years becomes more and more adapted to the low PO2, so that it causes fewer deleterious effects on the body. • it becomes possible for the person to work harder without hypoxic effects or to ascend to still higher altitudes.
PRINCIPAL MEANS BY WHICH ACCLIMATIZATION OCCURES • 1-Increased Pulmonary Ventilation—Role of Arterial Chemoreceptors • The respiratory centers are much more responsive to the peripheral chemoreceptor stimulus caused by the hypoxia
2-Increase in Red Blood Cells and Hemoglobin ConcentrationDuring Acclimatization. • The blood volume also increases, often by 20 to 30 per cent, and this increase times the • increased blood hemoglobin concentration gives an increase in total body hemoglobin of 50 or more percent. So, hematocrit increases.
3-Increased Diffusing Capacity After Acclimatization. • Normal diffusing capacity for oxygen through the pulmonary membrane is 21 ml/mm Hg/min. increase is due to: • 1-increased pulmonary capillary blood volume, which expands the capillaries • 2-An increase in lung air volume, which expands the surface area of the alveolar-capillary interface still more. • 3-An increase in pulmonary arterial blood pressure;
Increased Tissue Capillarity. • Increased tissue capillarity (or angiogenesis).
5-Cellular Acclimatization • cell mitochondria and cellular oxidative enzyme systems are slightly more plentiful than in sea-level inhabitants. So, tissues can extract more oxygen.
Chronic Mountain Sickness • (1) the red cell mass and hematocrit become exceptionally high, • (2) the pulmonary arterial pressure becomes elevated even more than the normal elevation that occurs during acclimatization, • (3) the right side of the heart becomes greatly • enlarged, • (4) the peripheral arterial pressure begins to fall, • (5) congestive heart failure ensues, • (6) death often follows unless the person is removed to a lower altitude.
First, the red cell mass becomes so great that the blood viscosity increases severalfold; this increased viscosity tends to decrease tissue blood flow so that oxygen delivery also begins to decrease. • Second, the pulmonary arterioles become vasoconstrictedbecause of the lung hypoxia. Because all the alveoli are now in the low-oxygen state, all the arterioles become constricted, the pulmonary arterial pressure rises excessively, and the right side of the heart fails. • Third, the alveolar arteriolar spasm diverts much of the blood flow through nonalveolarpulmonary vessels, thus causing an excess of pulmonary shunt blood flow where the blood is poorly oxygenated; this further compounds the problem. • Most of these people recover within days or weeks when they are moved to a lower altitude
Effects of prolonged stay in space • (1) decrease in blood volume, • (2)decrease in red blood cell mass, • (3) decrease in muscle strength and work capacity, • (4) decrease in maximum cardiac output, • (5) loss of calcium and phosphate from the bones, as well as loss of bone mass. • Most of these same effects also occur in people who lie in bed for an extended period of time.
Cardiovascular, Muscle, and Bone “Deconditioning” DuringProlonged Exposure to Weightlessness • Astronautson space flights lasting several months have shown 1-loss of as much 1.0 percent of their bone mass each month even though they continue to exercise. • 2-Atrophy of cardiac and skeletal muscles • also occurs during prolonged exposure to a microgravity environment. • 3-One of the most serious effects is cardiovascular • “deconditioning”, which includes decreased work • capacity, reduced blood volume, impaired baroreceptor • reflexes, and reduced orthostatic tolerance. Limited ability to stand upright.
4-They are also susceptible to bone fractures and may require several • Weeks to return to pre-flight cardiovascular,bone, and muscle fitness. • Prevention: • Application of intermittent “artificial gravity” caused by short periods (e.g., 1 hour each day) of centrifugal acceleration of the astronauts while they sit in specially designed short-arm centrifuges that create forces of upto 2 to 3 G.