Download
1 / 17
200 likes | 462 Views
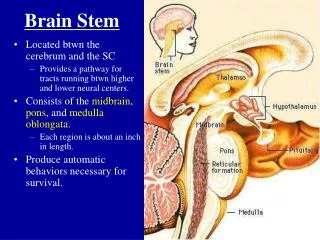
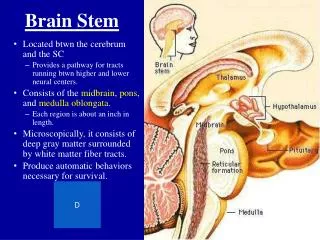
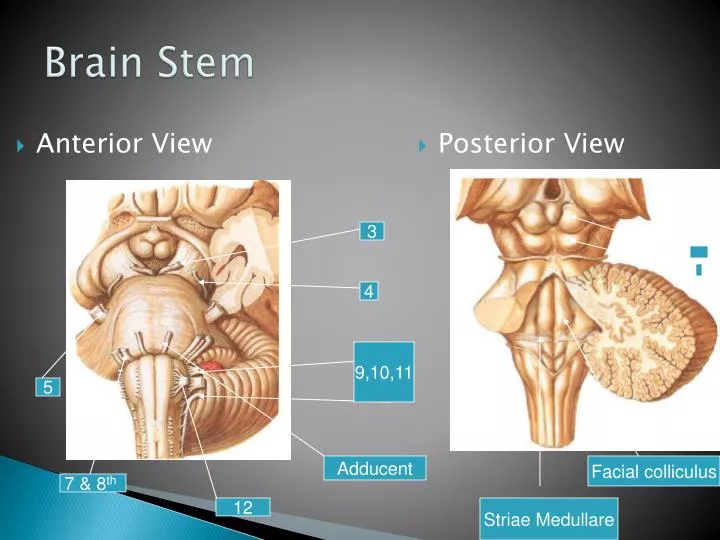
Anterior View. Posterior View. Brain Stem. 3. 4. 9,10,11. 5. Adducent. Facial colliculus. 7 & 8 th. 12. Striae Medullare. Brain Stem. Case.

E N D
Anterior View Posterior View Brain Stem 3 4 9,10,11 5 Adducent Facial colliculus 7 & 8th 12 Striae Medullare
Case • A 58 year old man suddenly fell on the floor and he was unable to rise from the floor. He felt his speech is very thick and he felt his limbs were paralyzed. • Neurologic examination week s later showed that he had a spastic paralysis of his left limbs with increased tone and exaggerated deep tendon reflexes. Motor examination of the face was normal, however upon protrusion, the tongue pointed toward her right side; the right side of his tongue was atrophic.
Case Cont.. • The sensory exam indicated that pain and temperature was bilaterally normal from the body and face but there was loss of proprioception from the left lower extremity. Examination of other cranial nerves was normal.
Case 2 • A 30-year-old man was admitted to the emergency room because of a severe headache. The patient says that the headache, which seems localized to the area behind his ears, it been intermittent but persistent since he was involved in the beach volleyball game while on vacation. Shortly after he returned from his vacation, he made an appointment with his family physician because he was worried about the headache and the fact that he had developed clumsiness.
Physical examination reveals mild hoarseness and some difficulty swallowing oral secretions. The left side of his face is affected by Horner’s syndrome,. He has decreased sensitivity to lighttouch on the left side of his face, flattening of the left nasolabial fold, and paresis of the left soft palate. Finger to nose testing shows left sided dysmetria. There is diminished pain and thermal sensation on the right side of the rest of the body. There is no Babinski reflex, and the remainder of the motor and sensory examination is normal
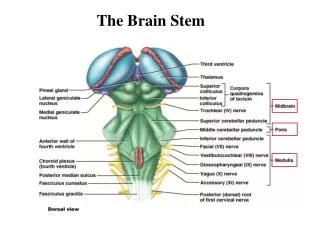
Medulla Oblongata • Nuclei in the medulla are associated w/ autonomic control, cranial nerves, and motor/sensory relay. • Autonomic nuclei: • Cardiovascular centers • Cardioinhibitory/cardioacceleratory centers alter the rate and force of cardiac contractions • Vasomotor center alters the tone of vascular smooth muscle • Respiratory rhythmicity centers • Receive input from the pons • Additional Centers • Emesis, deglutition, coughing, hiccupping, and sneezing
Medullary syndromes • Medial • Lateral medullary syndromes
Medial Medullary Syndrome • Alternating hemiplegia • Cranial Nerves • Tongue Paralysis -Hypoglossal Nerve • Motor Pathways • Contralateral Spastic Paralysis -- Pyramids • Sensory Pathways • Contralateral loss Fine Touch and Proprioception -- Medial Lemniscus
Hypoglossal Palsy Lower Motor Neuron Syndrome Deviation of Tongue to affected side Atrophy of Tongue Muscles
Lateral medullary syndrome(Wallenberg's syndrome) • This is the commonest of the brain stem strokes. Involvement of the spinothalamic tract results in contralateral loss of pain and temperature sensation below the neck. • Involvement of the descending nucleus and tract of V results in loss of pain and temperature sensation on the face ipsilateral to the lesion.
Lateral medullary syndrome • Involvement of descending autonomic fibers results in an ipsilateral Horner's syndrome (ptosis, meiosis, and anhidrosis). Involvement of the nucleus ambiguus causes palatal weakness and dysphagia. • Involvement of the inferior cerebellar peduncle (restiform body) causes ipsilateral ataxia. • Alternating hemianaesthesia