Download
1 / 1
10 likes | 235 Views
A phase I dose escalating study of intensity modulated radiation therapy (IMRT) for the treatment of glioblastoma multiforme (GBM) ( #1008). V. Stieber 1 , S. Tatter 2 , J. Lovato 5 , T. Ellis 2 , A. deGuzman 1 , W. Hinson 1 , W. Kearns 1 ,

E N D
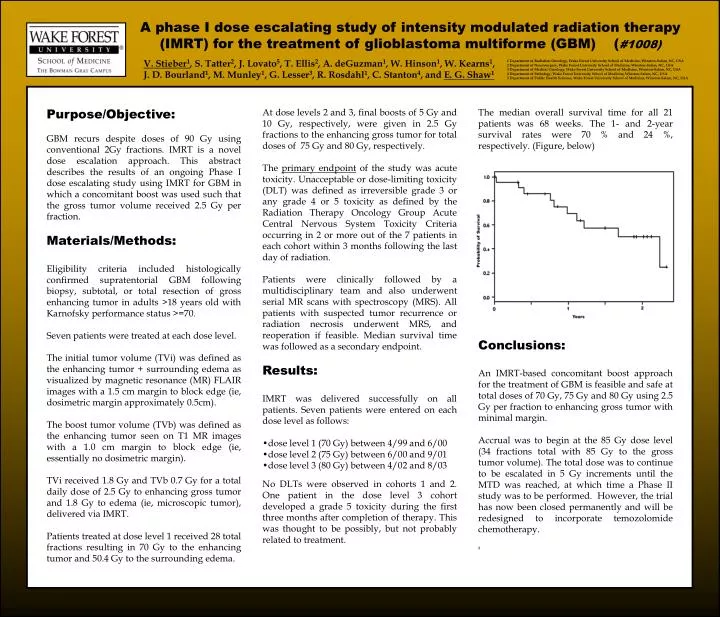
A phase I dose escalating study of intensity modulated radiation therapy (IMRT) for the treatment of glioblastoma multiforme (GBM) (#1008) V. Stieber1, S. Tatter2, J. Lovato5, T. Ellis2, A. deGuzman1, W. Hinson1, W. Kearns1, J. D. Bourland1, M. Munley1, G. Lesser3, R. Rosdahl1, C. Stanton4, and E. G. Shaw1 1 Department of Radiation Oncology, Wake Forest University School of Medicine, Winston-Salem, NC, USA 2 Department of Neurosurgery, Wake Forest University School of Medicine, Winston-Salem, NC, USA 3 Department of Medical Oncology, Wake Forest University School of Medicine, Winston-Salem, NC, USA 4 Department of Pathology, Wake Forest University School of Medicine, Winston-Salem, NC, USA 5 Department of Public Health Sciences, Wake Forest University School of Medicine, Winston-Salem, NC, USA Purpose/Objective: GBM recurs despite doses of 90 Gy using conventional 2Gy fractions. IMRT is a novel dose escalation approach. This abstract describes the results of an ongoing Phase I dose escalating study using IMRT for GBM in which a concomitant boost was used such that the gross tumor volume received 2.5 Gy per fraction. Materials/Methods: Eligibility criteria included histologically confirmed supratentorial GBM following biopsy, subtotal, or total resection of gross enhancing tumor in adults >18 years old with Karnofsky performance status >=70. Seven patients were treated at each dose level. The initial tumor volume (TVi) was defined as the enhancing tumor + surrounding edema as visualized by magnetic resonance (MR) FLAIR images with a 1.5 cm margin to block edge (ie, dosimetric margin approximately 0.5cm). The boost tumor volume (TVb) was defined as the enhancing tumor seen on T1 MR images with a 1.0 cm margin to block edge (ie, essentially no dosimetric margin). TVi received 1.8 Gy and TVb 0.7 Gy for a total daily dose of 2.5 Gy to enhancing gross tumor and 1.8 Gy to edema (ie, microscopic tumor), delivered via IMRT. Patients treated at dose level 1 received 28 total fractions resulting in 70 Gy to the enhancing tumor and 50.4 Gy to the surrounding edema. • At dose levels 2 and 3, final boosts of 5 Gy and 10 Gy, respectively, were given in 2.5 Gy fractions to the enhancing gross tumor for total doses of 75 Gy and 80 Gy, respectively. • The primary endpoint of the study was acute toxicity. Unacceptable or dose-limiting toxicity (DLT) was defined as irreversible grade 3 or any grade 4 or 5 toxicity as defined by the Radiation Therapy Oncology Group Acute Central Nervous System Toxicity Criteria occurring in 2 or more out of the 7 patients in each cohort within 3 months following the last day of radiation. • Patients were clinically followed by a multidisciplinary team and also underwent serial MR scans with spectroscopy (MRS). All patients with suspected tumor recurrence or radiation necrosis underwent MRS, and reoperation if feasible. Median survival timewas followed as a secondary endpoint. • Results: • IMRT was delivered successfully on all patients. Seven patients were entered on each dose level as follows: • dose level 1 (70 Gy) between 4/99 and 6/00 • dose level 2 (75 Gy) between 6/00 and 9/01 • dose level 3 (80 Gy) between 4/02 and 8/03 • No DLTs were observed in cohorts 1 and 2. One patient in the dose level 3 cohort developed a grade 5 toxicity during the first three months after completion of therapy. This was thought to be possibly, but not probably related to treatment. The median overall survival time for all 21 patients was 68 weeks. The 1- and 2-year survival rates were 70 % and 24 %, respectively. (Figure, below) Conclusions: An IMRT-based concomitant boostapproach for the treatment of GBM is feasible and safe at total doses of 70 Gy, 75 Gy and 80 Gy using 2.5 Gy per fraction to enhancing gross tumor with minimal margin. Accrual was to begin at the 85 Gy dose level (34 fractions total with 85 Gy to the gross tumor volume). The total dose was to continue to be escalated in 5 Gy increments until the MTD was reached, at which time a Phase II study was to be performed. However, the trial has now been closed permanently and will be redesigned to incorporate temozolomide chemotherapy. 2