Download
1 / 33
330 likes | 469 Views
Mortality Among Very Low Birthweight Infants in Hospitals Serving Minority Populations. Support Provided by: UCLA-Drew EXCEED Program (AHRQ), RWJ Minority Medical Faculty Development Program, and UCLA-RCMAR Center (NIA). Leo Morales, M.D., Ph.D. Assistant Professor, UCLA. AcademyHealth

E N D
Mortality Among Very Low Birthweight Infants in Hospitals Serving Minority Populations Support Provided by: UCLA-Drew EXCEED Program (AHRQ), RWJ Minority Medical Faculty Development Program, and UCLA-RCMAR Center (NIA) Leo Morales, M.D., Ph.D. Assistant Professor, UCLA AcademyHealth June 7, 2004
Key Collaborators • Jeanette Rogowski, Ph.D., University of Medicine and Dentistry of New Jersey andRAND • Douglas Staiger, Ph.D., Dartmouth University • Jeffery Horbar, M.D., The Vermont Oxford Network (VON) • Joe Carpenter, M.S., VON • Mike Kenny, M.A., VON • Jeff Geppert, M.A., National Bureau of Economic Research
Hospital Characteristics and Patient Outcomes • Worse outcomes are associated with: • Rural hospitals (Kahn, 1994) • Non-teaching hospitals (Kuhn, 1994; Polanczyk, 2002; Taylor, 1999; Kahn, 1994) • For-profit hospitals (Hartz, 1989; Haas, 2003) • Lower expenses per admission (Burstin, 1993) • Minority-serving hospitals (Brennan, 1991) • Low volume and lower level of care (Phibbs, 1996) • Little is known about the relationship of minority-serving hospital status to infant mortality
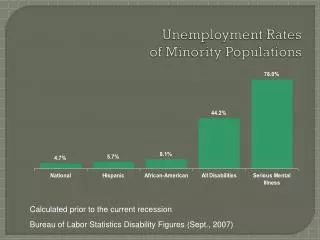
Trends in Infant Mortality • Overall, infant mortality is decreasing for black and white infants • However, the disparity between black and white infant mortality remains constant and maybe increasing (MacDorman, 2002) • Black infant mortality 14.1 per 1,000 live births • White infant mortality 5.7 per 1,000 live births • Eliminating the racial disparity in infant mortality is one of six target areas in the Health People 2010 initiative
Very Low Birthweight Infants • Definitions • Low birthweight (LBW): <2500 grams • Very low birthweight (VLBW): <1500 grams • Small but high risk infant population • LBW infants account for 7.6% of live births but 66% of all infant deaths (MacDorman, 2002) • VLBW infants account for 1.4% of live births but 52% of all infant deaths (MacDorman, 2002)
Research Questions • Do VLBW infants treated by minority-serving hospitals have similar neonatal mortality as those treated by other hospitals? • Do hospital characteristics and process of care variables explain differences in neonatal mortality between minority-serving hospitals and other hospitals? • Are black and white infants treated by minority-serving hospitals at similar risk for neonatal mortality?
Primary Data Source • 1995-2000 Vermont Oxford Network (VON) • 332 hospitals • 40% of US hospitals with NICUs • 50% of VLBW infants in US • Abstracted medical records • Mortality outcomes • Case-mix variables • Process of care • Institutional survey of participating hospitals • NICU level of care
Additional Data Sources • American Hospital Association Annual Survey of Hospitals • Hospital characteristics • 1990 United States Census • Maternal income and education
Study Subjects • VLBW infants between 500g and 1500g • White infants (n= 49,132) • Black (n=24,918) • Inborn infants only
Outcome Variable • Neonatal mortality • Mortality in the first 28 days after birth • Mortality ascertained through transfers until discharge home
Main Explanatory Variable:Hospital Minority-Serving Status • Hospitals assigned to 1 of 3 categories based on the proportion of infants treated between 1995 and 2000 who were Black • % VLBW black infants = VLBW black infants / VLBW black and white infants
Explanatory Variables:Case-Mix Variables • Gestational age (+ gestational age squared)* • Birthweight* • Small for gestational age • Congenital malformation • Multiple birth • Any prenatal care • 1-minute APGAR • Sex • Race • Vaginal delivery • Maternal income and education based on census
Explanatory Variables:Hospital Variables • Geography • Region • Urban setting of >1,000,000 • NICU characteristics • Level of care • Volume • Hospital characteristics • Ownership • Teaching status • Percent Medicaid admissions • Expenditures per admission • Average maternal income and education based on census
Explanatory Variables:Process of Care Variables • Indicator variables: • Treatment with surfactants • Treatment with antenatal steroids
Statistical Models • Descriptive analysis • Infants by case-mix, hospital, and process of care variables • Stratified regression by race • %black + case-mix • Pooled regression • Model 1: %black + case-mix • Model 2: %black + case-mix + hospital • Model 3: %black + case-mix + hospital + process of care
Estimation Methods • Maximum-likelihood logistic regression models • Robust standard errors • Clustering of infants within hospitals • STATA 8.0
Stratified Logistic Regressions:Neonatal Mortality on Case-Mix Variables Note. Models include year dummies. *p<0.05 **p<0.01
Pooled Regressions:Neonatal Mortality on Hospital and Case-Mix Variables Note. Models include case-mix model and year dummies. *p<0.05 **p<0.01
Thought Experiment-1 • What if black infants were treated by the three categories of hospitals we studied (e.g., <15% black, 15% to 35% black, >35% black) in the same proportions as white infants? • Black infant mortality would drop by 8.5%
Thought Expereiment-2 • What if neonatal mortality at hospitals where 15% or more of the treated infants were black were the same as hospitals where <15% of the infants treated were black? • 10% lower for white infants • 22% lower for black infants
Conclusions • Minority-serving hospitals had higher neonatal mortality than other hospitals • The difference in neonatal mortality between minority-serving and other hospitals was not explained by the hospital variables or process of care variables • Neonatal morality was similarly elevated for black and white VLBW infants treated by minority-serving hospitals
Implications • Minority-serving hospitals may provide worse quality of care than other hospitals • Hospital-level factors may be more important in understanding disparities in care than individual characteristics such as infant race per se, at least among VLBW infants • Disparities in infant mortality nationally might be reduced by improving care for VLBW infants at minority-serving hospitals
Potential Explanations for Results • Staffing patterns • Nurse-to-patient ratio • Board-certified specialists • Maternal characteristics: smoking, drug and alcohol use • Mediated by infant severity of illness • Infant characteristics in minority-serving similar to other hospitals • Maternal income and education had no effect • Unmeasured severity of illness • VON risk adjustment ROC=0.88 • SNAP ROC=0.73 to 0.91
Study Generalizability • Compared with all US hospitals, VON hospitals are: • More likely to be private non-profit • Teaching hospitals • Children’s hospitals • More NICU beds • Compared with all VLBW infants in US, VLBW infants treated by VON hospitals are: • Differed in terms of birthweight but not gestational age
Secondary Analyses • Do the effects of risk-adjustment vary by race? • Insignificant case-mix*race interactions • Do the effects of minority-serving status vary by race? • Insignificant percent black*race interactions • Do the effects of hospital variables vary by percentage black infants treated? • Insignificant percent black*hospital characteristic interactions