Download
1 / 47
510 likes | 887 Views
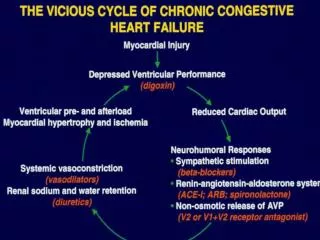
Prof. Denis Agostini Caen University Hospital France BARCELONA 2009. RISK STRATIFICATION IN HEART FAILURE ROLE OF CARDIAC I-123- MIBG IMAGING :. Most commonly used tracers for assessment of cardiac pre-synaptic processes. Pre-synaptic. Adapted from Carrio I. J Nucl Med 2001; 42:1062–1076.

E N D
Prof. Denis Agostini Caen University Hospital France BARCELONA 2009 RISK STRATIFICATION IN HEART FAILUREROLE OF CARDIAC I-123- MIBG IMAGING :
Most commonly used tracers for assessmentof cardiac pre-synaptic processes Pre-synaptic Adapted from Carrio I. JNucl Med 2001; 42:1062–1076
MIBG & HEART FAILURE MILESTONE (1992-2009) Retro and prospective Studies in US and Europe MIBG and pheo neuroblastoma MIBG prospective studies results 2002 1992 2009 2008 European Retrospective Study Agostini et al Verberne et al EJNMMI Meta-analysis Verberne et al Eur Heart J Arrhythmia Bax J Circ Cardiovasc Imaging 2008 Impact of therapy on neuronal Function (exercise, BB, ACI, Sartan) and CRT Prognosis Merlet et al J Nucl Med
100 100 H/M>120% H/M>120% H/M<120% H/M<120% DCM, n=90 IDCM, n=112 0 25 0 24 Elapsed time in months Elapsed time in months JNM 1992 J Nucl Med 1992 Survival rate Survival rate
Cardiac Sympathetic Denervation is more EXTENSIVE than the Infarct Size 99mTc SPECT Infarct Size 123I-mIBG 15.2 %LV 59.3 %LV Matsunari et al. Circ 2000
Patients with heart failure: • Prognosis stratified by semi-quantitative 123I-MIBG myocardial • parameters (i.e. early H/M, late H/M and myocardial washout). • Outcome measure: • Cardiac death • Cardiac event (combination of cardiac death, myocardial infarction, heart transplantation and hospital admission due to progression of heart failure).
Conclusion of MIBG meta-analysis • Reduced late H/M or increased myocardial MIBG washout is associated with a poorer prognosis • In general poor quality of performed studies : • Single center studies (Europe-Japan) • Small samples of patients in each study • No standardization of imaging methodology (collimator, HM or WO ratios…) • No MIBG-SPECT studies • No MPI
Eur J Nucl Med Mol Imaging 2008 • To demonstrate the feasibility of using a standardized methodology for analysis of cardiac 123I-mIBG scintigraphy performed at multiple centres • To demonstrate the utility of 123I-mIBG uptake as measured by the heart–to-mediastinum (HMR) ratio for identifying subjects with NYHA Class II-IV CHF who experience a Major Cardiac Events (MCE) during a 24-month follow-up period
Death Rate vs MIBG uptakeNYHA II-III Subjects, LVEF ≤ 35% (n=182) n 38 78 43 23 2-Yr Death Rate (%) * NO MCE!! *Including 6 deaths post-transplant and 1 post-CABG. p<0.05 H/M Ratio
Prognostic Significance of [123I]mIBG Myocardial Scintigraphy in Heart Failure Patients: Results from the Prospective Multicenter International ADMIRE-HF Trial Arnold F. Jacobson, MD, PhD Roxy Senior, MD, DM, FRCP, FESC, FACC Fred Weiland, MD Harish Chandna, MD Denis Agostini, MD, PhD for the ADMIRE-HF* investigators (ACC 2009) *ADMIRE-HF: AdreView Myocardial Imaging for Risk Evaluation in Heart Failure
ADMIRE HF: a landmark study • Integration of two identicalopen-label Phase III trials (MBG311 and MBG312) • Multicenter study 96 centres(35 EU, 57 US, 4 Canada) • July 2005 to September 2008 • 985 heart failure patients – 110 age-matched control ADMIRE-HF: AdreView Myocardial Imaging for Risk Evaluation in Heart Failure
Primary Objective of ADMIRE-HF: To demonstrate the prognostic usefulness of assessment of myocardial sympathetic innervation, as determined by the heart to mediastinum (H/M) ratio on planar AdreView imaging as either normal (≥1.6) or abnormal (<1.6), for identifying HF subjects at higher risk of experiencing an adverse cardiac event.
Primary eligibility criteria NYHA II/III HF (ischemic or non-ischemic) LVEF≤35% Guidelines-based management including ACE inhibitors/ARBs and beta blockers No previous defibrillation to treat a ventricular arrhythmic event METHODS
Composite Primary Endpoint First occurrence of any of the following 3 categories of adverse cardiac events 1. HF Progression: Progression of HF stage (NYHA II to III or IV; NYHA III to IV). 2. Arrhythmic Event: Sustained ventricular tachyarrhythmia Appropriate ICD discharge Aborted cardiac arrest 3. Terminal Cardiac Event: Cardiac death METHODS
Demographics and Clinical Characteristics 961 HF subjects were evaluable for efficacy
Primary Endpoint Events 237 subjects (25%) had an adverse cardiac event.
Secondary Endpoint Events 52 subjects had a second event of a different category following a first event of HF progression or arrhythmia. *23 SCD, 24 HF death, 5 MI, 1 cardiac surgery complication
Composite Primary Endpoint 40 p<0.0001 H/M<1.60 30 Cumulative Rate (%) 20 H/M≥1.60 10 0 H/M<1.60 760 629 441 241 67 H/M≥1.60 201 178 141 85 28 Months Follow-up
Heart Failure Progression H/M<1.60 30 p=0.001 20 Cumulative Rate (%) H/M≥1.60 10 0 Months Follow-up
All Arrhythmic Events 30 p=0.002 20 Cumulative Rate (%) H/M<1.60 10 H/M≥1.60 0 H/M<1.60 760 678 503 299 84 H/M ≥1.60 201 171 116 95 29 Months Follow-up
Cardiac Death 30 p=0.001 20 Cumulative Rate (%) H/M<1.60 10 H/M≥1.60 0 H/M<1.60 760 701 536 328 94 H/M≥1.60 201 176 121 99 32 Months Follow-up
Representative ADMIRE-HF Subjects Based upon the H/M ratios, 2-year cardiac mortality risk for patient 1 is 10 times that of patient 3. 1 2 3 65 y/o M NYHA 2 DCM LVEF=25% H/M=0.96 51 y/o M NYHA 2 ICM LVEF=33% H/M=1.38 64 y/o M NYHA 2 ICM LVEF=30% H/M=1.67 No event Died at 8 mo HF Progression Died at 8 mo, SCD (No ICD)
Composite Primary Endpoint 50 P=0.0004 LVEF<30%, H/M<1.60 40 30 Cumulative Rate (%) LVEF<30%, H/M≥1.60 20 10 0 Months Follow-up
Conclusions 1. ADMIRE-HF achieved its primary efficacy objective, demonstrating the prognostic value of the AdreView uptake (H/M ratio <1.60 vs ≥1.60 on sympathetic innervation imaging) for identifying higher vs lower risk for adverse cardiac events in HF patients with LVEF≤35%. 2. The prognostic value of AdreView imaging was demonstrated for each of the categories in the composite endpoint (HF progression, arrhythmic events, cardiac death). 3. Between the highest and lowest risk subpopulations (H/M<1.20 and H/M≥1.60), there was a tenfold difference in 2-year cardiac mortality rate.
CONCLUSION STRENGTHS: • Address the crucial unmet need of risk-stratifying heart failure pts • Several clinical trials in Europe and US using MIBG (700 €) OPPORTUNITIES: • Increasing # heart failure patients • Prophylactic use of ICD (> 50 000€) • Payers pressure • New technology for dual perfusion and MIBG-SPECT (ALCYONE-CZT)
Adreview Leiden Study, the impact on sudden death risk stratification and ICD implantation J Bax et al
Sudden Cardiac Arrest Statistics • One of the most common causes of death in developed countries: Incidence(cases/year) Survival Worldwide 3,000,0001 <1% U.S. 450,0002 5% W. Europe 400,0003 <5% • High recurrence rate
Primary Prevention Post-MI Trials: Reduction in Mortality with ICD Therapy 73% 75% 61% 55% 54% % Mortality Reduction w/ ICD Rx 31% 1 2 3, 4 27 Months 39 Months 20 Months
Annual ICD implants per million inhabitants Europe and USA USA Europe Updated from S. Nisam, 2000
2008 AHA/ACC/HRS guidelinesfor ICD implantation in primary prevention • Heart failure – NYHA II / III • ACS, MI > 40 days • Revascularisation > 90 days • LVEF ≤35%
Primary prevention Leiden registry N= 941, 80% male, age 63 ± 11 years all CAD, 83% previous MI LVEF 29±12% Treated with ICD Follow-up 31 ± 24 mth ICD therapy 66% 34% - +
What is the pathophysiological substrate for SCD in chronic CAD? • Depressed LVEF (scar) • Previous MI (scar) • Ischemia (jeopardized) • Dysfunctional but viable tissue (jeopardized) Burger vd Borg Circ 2003
MIBG Leiden Study Prediction of ICD therapy by mIBG imaging: Could mIBG imaging be the gatekeeper for ICD implantation in primary prevention of sudden death?
Study Population (n = 116) 116 consecutive patients referred for ICD implantation based on guidelines for primary prevention
Study Protocol Before ICD implantation: 123-I MIBG scintigraphy Planar and SPECT Early and delayed imaging 99m-Tc Tetrofosmin perfusion imaging Stress-rest protocol (adenosine)
MIBG Scintigraphy Planar imaging Early Heart /Mediastinum ratio Late Heart /Mediastinum ratio Cardiac washout rate
MIBG Scintigraphy SPECT imaging Early summed defect score Late summed defect score
Perfusion Imaging Resting 99m-Tc Tetrofosmin Summed rest score Stress 99m-Tc Tetrofosmin Summed stress score Summed difference score 123-I MIBG/perfusion mismatch score
Endpoints Clinical Follow-up From ICD implantation to first documented: Appropriate ICD therapy (prim endpoint) ATP or ICD shock induced by ventricular tachyarrhythmia ICD therapy + Cardiac mortality (sec endpoint)
Study Protocol Primary endpoint (n = 24) Appropriate ICD therapy Secundary endpoint (n = 32) Composite of appropriate ICD therapy or cardiac death
Predictors for ICD therapy (prim endpoint)- Imaging variables
Predictors for ICD therapy or cardiac death (sec endpoint)– imaging variables
Case example: 75-year old male patient ICD implantation, LVEF 28%received ICD therapy Rest Perfusion imaging Delayed MIBG imaging
Cumulative event rate for ICD therapy (n = 24) Cumulative event rate 79% vs. 5% 4-year follow-up data
Cumulative event rate for ICD therapy or cardiac death (n = 32) Cumulative event rate 83% vs. 10% 4-year follow-up data
Conclusion • The extent of denervated myocardium is related to induction of ventricular arrhythmias • Late MIBG SPECT defect size is the main predictor for ventricular arrhythmias in patients with cardiomyopathy undergoing ICD implantation for primary prevention of sudden death • MIBG may be used as gatekeeperfor ICD selection