Download
1 / 24
1k likes | 5.06k Views
Cardiac Tamponade. Dr. Mohammad AlGhamdi Consultant cardiologist King AbdulAziz Cardiac Center National Guard- Riyadh. Cardiac Tamponade. Life threatening Cardiac compression syndrome Due to pericardial fluid accumulation. Predisposing conditions.

E N D
Cardiac Tamponade Dr. Mohammad AlGhamdi Consultant cardiologist King AbdulAziz Cardiac Center National Guard- Riyadh
Cardiac Tamponade • Life threatening • Cardiac compression syndrome • Due to pericardial fluid accumulation
Predisposing conditions 60% of cases have known underlying conditions Neoplasm-related conditions Pericarditis (viral, uremic, TB, SLE,…) Trauma (medical & non-medical) Unrelated to effusion size, but to the rate of accumulation one-third of asymptomatic large chronic effusions develop unexpected cardiac tamponade
Tamponade pathophysiology Pathological process Mechanical Hemodynamic Clinical Echo Low cardiac output state due to reduced cardiac filling. Echo/Doppler findings attributed to hemodynamic abnormalities. Pericardial pressure equal to or exceeds intracardiac pressure. External mechanical compression.
Clinical approach + pericardial effusion Hemodynamic instability Clinical picture Basic investigations Imaging studies SOB Tachycardia Low BP High JVP Diminished HS Pulsus paradoxus Clear lungs ECG CXR Trans-thoracic echo TEE, CT scan, MRI
Limitations of clinical assessment Diminished HS Hypotension Low voltage EKG Pulsus Paradoxus PRESENT Asthma/COPD P. Embolism CHF Mitral Stenosis Hypovolemia Ascites Obesity ABSENT Hypotension P. adhesions AR ASD RVH Sensitivity <50% Dyspnea Tachycardia Elevated JVP Pulsus Paradoxus Cardiomegaly on CXR Sensitivity = 70%
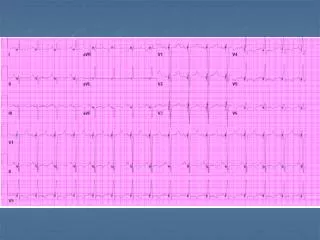
Low voltage Electrical alternans Basic investigations • Enlarged cardiac silhouette
CT or MRI Effusions measured by CT/MRI tend to be larger than in echocardiography
Just remember that … √ X • Tamponade is a clinical description not an echo diagnosis • Echo findings would support or refute clinical suspicion
Detecting Pericardial Effusion Echo-free space surrounding the heart Variable degrees of severity
Common Left pleural effusion Loculated Pericardial effusion Intrapericardial hematoma Epicardial fat pads Rare Pericardial cyst Desc. aortic aneurysm LV pseudoaneurysm Hiatus hernia Massive LAE Differential diagnosis of pericardial echo-free space
Important landmarks • Pericardial effusion is seen anterior to the descending aorta in PLA view • Left pleural effusion is posterior to the descending aorta
Tamponade by 2-D echo Pericardial effusion Heart swinging (chronic) Late RA diastolic collapse Early RV diastolic collapse Dilated IVC with reduced collapsibility
RA collapse • RA Inversion (collapse) • Begins in late diastole and continues into systole • Sensitive but not specific for clinical tamponade • Increased specificity if lasting >1/3 of systole • Brief inversion can occur without clinical tamponade
RV collapse • Occurs in early diastole • Duration of collapse is proportional to the severity • Indicates impending or existing clinical tamponade
Limitations of RV collapse • May be affected by: • Intravascular volume • Low pressure tamponade • RV Pressure/volume load • RVH and PHTN • ASD, TR, PI • RV compliance • Ischemia, Trauma, Pericardial adhesions
Tamponade by Doppler flow • Exaggerated respiratory variations • Inspiration: • Tricuspid flow increases • Mitral flow decreases • Expiration: • Tricuspid flow decreases • Mitral flow increases Mitral peak flow velocity variations of >25% Tricuspid peak flow velocity variations of >45%
Doppler timing 80-40÷80= 50% 120-75÷120= 38%
Hepatic vein flow Mitral inflow HV flow
Echo-guided perecardiocentesis • Confirm presence and hemodynamic effect of pericardial effusion • Check the window of maximum fluid collection (apical or subcostal) • Measure the depth from transducer (skin) to effusion
Echo-guided perecardiocentesis • Guide the operator for the needle direction • Confirm the presence of catheter in pericardial space • Check mechanical and hemodynamic improvement after drainage • Assess the residual pericardial effusion • Surgical drainage for post op collection/hematoma
Echo cases of tamponade To follow ….