Download
1 / 45
470 likes | 897 Views
Treating patients with epidermolysis bullosa. Jemima Mellerio Great Ormond Street Hospital and St John’s Institute of Dermatology London, UK. Treating patients with EB. EB and EB care in England and Wales What are the problems and what can we do about them?

E N D
Treating patients with epidermolysis bullosa Jemima Mellerio Great Ormond Street Hospital and St John’s Institute of Dermatology London, UK
Treating patients with EB • EB and EB care in England and Wales • What are the problems and what can we do about them? • Clinical trials in EB - what is there? • Why so few? • What could we do? • What is the way forward?
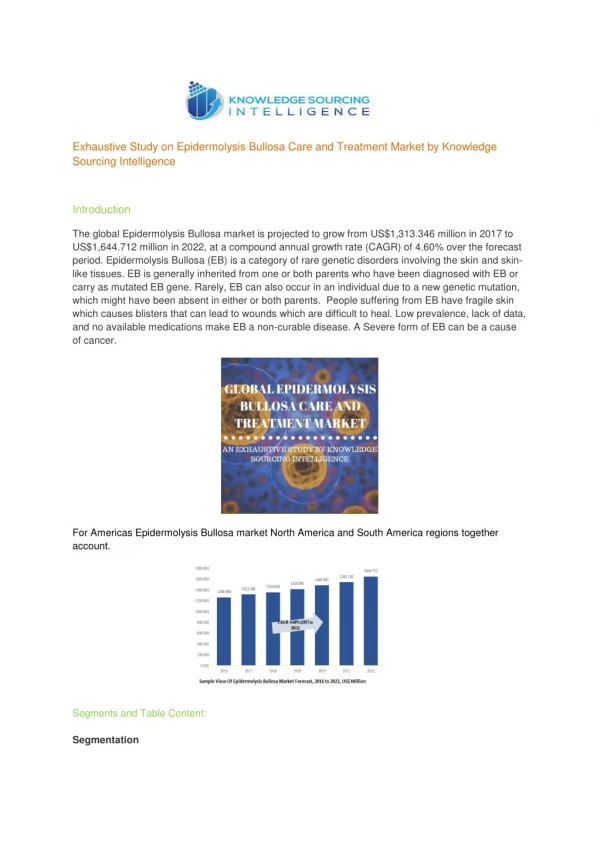
Epidermolysis bullosa (EB) • Group of inherited disorders • Skin +/- mucosal fragility • Variable severity • Variable non-cutaneous features • Overall incidence of approx 1 per 20,000 births • Estimated 5,000 with EB in UK
Epidermolysis bullosa (EB) • Result from mutations in genes encoding proteins at the dermal-epidermal junction • Latest classification: 13 different genes, many more clinical subtypes Fine J-D et al. J Am Acad Dermatol 2008; 58(6): 931-50
EB care in England and Wales • April 2002 NSCAG funding (National Specialist Commissioning Advisory Group) (now NCG) • Specialist centres to develop expertise in rare diseases • Funded by Department of Health • Reciprocal arrangements with Scotland and N Ireland
Ninewells & University of Dundee Great Ormond Street Hospital Birmingham Children’s Hospital St Thomas’ Hospital Robin Eady National Diagnostic EB Laboratory Heartlands Hospital EB care in England and Wales
Anaesthetist Oncologist Ophthalmologist Cardiologist Clinical geneticist Orthopaedic surgeon Dentist OT/hand therapist Dermatologist Paediatrician Dietician Physiotherapist Endocrinologist Plastic surgeon ENT surgeon Play therapist Gastroenterologist Podiatrist General surgeon Psychologist Haematologist Social worker Interventional radiologist Specialist nurse Symptom control team Microbiologist Obstetrician Urologist Multidisciplinary EB care
Wound healing EB: what are the problems and what can we do about them?
Infection EB: what are the problems and what can we do about them?
EB: what are the problems and what can we do about them? Hand contractures
EB: what are the problems and what can we do about them? Nutrition
EB: what are the problems and what can we do about them? Anaemia
EB: what are the problems and what can we do about them? Bone health
EB: what are the problems and what can we do about them? Airways
EB: what are the problems and what can we do about them? Eyes
EB: what are the problems and what can we do about them? Cancer
Pain GU problems Itch Delayed puberty Constipation Psychosocial Cardiomyopathy GO reflux
So many problems… So many interventions… So little evidence…
Clinical trials in EB - what is there? • Two double-blind placebo-controlled RCTs for oral tetracyclines in EB simplex • Small numbers (n=12 and n=21) • No evidence of benefit
Clinical trials in EB - what is there? • Two RCTs for topical interventions in EBS • 20% aluminium chloride hexahydrate (n=23) • 5% bufexamac cream (n=8) • No evidence for benefit from either
Clinical trials in EB - what is there? • One RCT with phenytoin vs placebo in recessive dystrophic EB • N=36 • No benefit from phenytoin
Clinical trials in EB - what is there? • Anecdotal reports and retrospective analyses • Small non-controlled trials with small numbers e.g. acceptability and efficacy of Urgotul dressings e.g. parenteral iron and erythropoietin for anaemia in EB • Tolerability of oral isotretinoin in patients with recessive dystrophic EB
Clinical trials in EB - what is there? • Pilot study of low dose trimethoprim in children with junctional and dystrophic EB
Clinical trials in EB - what is there? • Pilot study of low dose trimethoprim in children with junctional and dystrophic EB • Topical thymosin beta4 for wound healing in junctional and dystrophic EB
Clinical trials in EB - what is there? • Pilot study of low dose trimethoprim in children with junctional and dystrophic EB • Topical thymosin beta4 for wound healing in junctional and dystrophic EB • Efficacy of 2 different devices for improving microstomia in severe generalised recessive dystrophic EB
Clinical trials in EB - what is there? • Pilot study of low dose trimethoprim in children with junctional and dystrophic EB • Topical thymosin beta4 for wound healing in junctional and dystrophic EB • Efficacy of 2 different devices for improving microstomia in severe generalised recessive dystrophic EB
Clinical trials in EB - what is there? • Topical opioids for wound pain in EB • Low dose amitriptyline for chronic pain in children with EB
Clinical trials in EB - what is there? • Ex vivo gene therapy for non-Herlitz junctional and recessive dystrophic EB
Clinical trials - why so few? • EB is a rare disease especially if break down into subtypes…hard to get decent numbers • Validity of comparing different subtypes of EB? • Other variables e.g. temperature, infection, anaemia, age
Clinical trials - why so few? • Hard to get objective measures e.g. blister counts, wound healing
Clinical trials - why so few? • What would ‘normal’ healing rate be?
Clinical trials - why so few? • Could evaluate ‘before’ and ‘after’
Clinical trials - why so few? • More global measures e.g. pain diaries, QoL measures may not be sufficiently sensitive to detect real differences • Birmingham EB Severity Score • Sydney QoL EB index
Clinical trials - why so few? • May mean yet another intervention or treatment for patient and carers • May be higher drop outs due to other factors e.g. intercurrent illness • Extra visits for study may be unfeasible
Clinical trials - what to do? • Anaemia in severe forms of EB • Parenteral iron +/- erythropoietin
Clinical trials - what to do? • Osteoporosis in severe forms of EB • Effects of bisphosphonates on EB bone turnover • Potential benefits from low amplitude vibrating platforms
Clinical trials - what to do? • Cancer chemoprevention in recessive dystrophic EB • Trial of oral retinoids: tolerability and efficacy
Clinical trials - what to do? • Cancer management
Clinical trials - what to do? • Cancer management • Role of imiquimod for treatment of early in situ tumours or palliation
Clinical trials - what to do? • Cancer management • Role of Mohs micrographic surgery or sentinnel lymph node biopsy?
Clinical trials - what to do? • Cancer management • Role of newer chemotherapeutic agents e.g. EGFR inhibitors and tyrosine kinase inhibitors
Clinical trials - what to do? • Gene, cell and protein therapy EB gene Skin biopsy
Baseline Allogeneic fibroblasts Clinical trials - what to do? • Gene, cell and protein therapy
What is the way forward? • UK in privileged position • Large clinical centres for adults and children providing comprehensive multidisciplinary care • Most patients with more severe forms seen regularly at one of these centres • Links to excellent diagnostic services • Invaluable role of DebRA UK
What is the way forward? • UK multi-centre trials much needed • International collaboration is the way forward for more power and larger numbers • Already good communication and links between EB centres in EU and beyond • Need to overcome administrative and financial hurdles to enable clinical trials to be undertaken