Download
1 / 20
480 likes | 1.1k Views
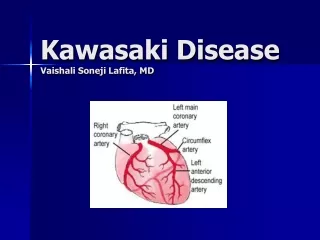
Kawasaki Disease . Morning Report 7/13/09. Kawasaki Disease. Acute febrile vasculitic syndrome of early childhood Affecting all blood vessels in the body but mostly medium and small vessels with a preferential involvement of the coronary arteries.

E N D
Kawasaki Disease Morning Report 7/13/09
Kawasaki Disease • Acute febrile vasculitic syndrome of early childhood • Affecting all blood vessels in the body but mostly medium and small vessels with a preferential involvement of the coronary arteries. • Exact etiology unknown but thought to be infectious in nature • Immune response thought to be oligoclonal or antigen driven
Epidemiology • Race: Japanese > Blacks, Polynesians, Filipinos > Whites • Gender: Male:Female~ 3:2 • Age: • 90-95% <10years old • Peak incident 18-24months
Diagnosis • Presence of 5 or more days of fever + 4 or more of the 5 principle clinical features
Changes in Lips and Oral Cavity (Erythema, Stawberry Tongue)
Other Clinical Findings • Arthritis/arthralgia • Irritability • Diarrhea, Vomiting, Abdominal Pain • Hepatomegally, Jaundice • Pleural Effusions, infiltrates • Stiff Neck secondary to aseptic meningitis
Incomplete or Atypical Kawasaki Disease • Children with unexplained fever for more than 5 days associated with 2-3 of the principle clinical features • More common in young infants • May be supported by laboratory evidence of systemic inflammation
Differential Diagnosis • Viral Infections (Measles, adenovirus, enterovirus, EBV) • Scarlet Fever • Staphylococcal scalded skin syndrome • Bacterial cervical lymphadenitis • Rocky Mountain Spotted Fever • Leptospirosis
Lab Studies • Moderate to high WBC count with left shift • Anemia • Elevated ESR, CRP • Thrombocytosis • Mild-Moderate elevation in transaminases • Sterile Pyuria
Differential Diagnosis cont… • Toxic Shock Syndrome • Drug Hypersensitivity • Steven-Johnson syndrome • Juvenile idiopathic arthritis • Juvenile Polyarteritis Nodosa • Mercury hypersensitivity reaction
Cardiac Imaging • Echocardiogram is critical for the evaluation of all patients suspected of having KD. • Baseline echo during acute stage to r/o coronary artery aneurysms and evidence of myocarditis, valvulitis, or pericardial effusion • Echo should be repeated in 2nd-3rd week of illness and again 1 month after (or once all lab values normalize) • Prior to treatment 20-25% of patients had Cardiac involvement with mortality rate 0.1-2% • With IVIG risk reduced to 5%
Treatment • Standard therapy is IVIG with Asprin • During the acute phase of illness • IVIG (2gm/kg) and • Asprin 80-100mg/kg /day • Continue high dose asprin until day 14 of illness if still afebrile • Continue asprin 3-5mg/kg/day until no evidence of coronary changes by 6-8 weeks
~10% fail to respond to initial IVIG therapy (persistence of fever after 36hrs) • Retreatment with IVIG at same dose recommended
Other Options • 3rd dose IVIG • Pulse Steroids (Methylprednisolone mg/kg for 2-3 hours qday x3days) • Infliximab (monoclonal ab against tumor necrosis factor) • Cyclophosphamide • Methotrexate
Long Term Follow Up • MI caused by thrombotis occlusion of abnormal coronary artery Is principle cause of death • Usually occurs within first year • Children at high risk need frequent ECHO evaluations • Small solitary aneurysms-long term asprin therapy • Giant aneurysms or multiple complex aneurysms-long term antiplatelet therapy and anticoagulation • Primary surgical management is coronary artery bypass graft