Download
1 / 70
700 likes | 1.07k Views
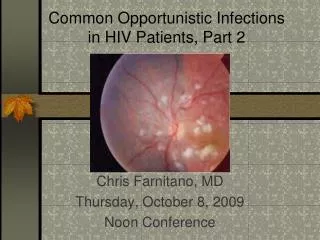
Common Opportunistic Infections in HIV Patients. Chris Farnitano, MD Monday, August 31, 2009 Noon Conference. Objectives. Discuss most common opportunistic infections (OIs): Dx and Rx Discuss immune reconstitution disease Review primary OI prophylaxis. Forms.

E N D
Common Opportunistic Infections in HIV Patients Chris Farnitano, MD Monday, August 31, 2009 Noon Conference
Objectives • Discuss most common opportunistic infections (OIs): Dx and Rx • Discuss immune reconstitution disease • Review primary OI prophylaxis
What are the most common OI’s? • Cohort Studies in pre-triple therapy era: • Candida • Pneumocystis Carinii • Cytomegalovirus • Mycobacterium Avium Complex • Pneumocystis - second episode • Toxoplasmi gondii • Herpes zoster
Causes of death, PHC HIV clinic • 2007-9 • RH: Crypto meningitis • TW: street drug overdose • SA: sepsis, pneumonia and massive hemoptysis • DW: metastatic prostate ca • RP: CVA, laryngeal ca • VA: PML (progressive multifocal leukencephalopathy) • AM: bacterial pneumonia, ETOH cirrhosis, wasting
OIs diagnosed, PHC HIV clinic • 2005-9 • PCP pneumonia • Esophageal Candidiasis • Herpes Simplex • Herpes Zoster • M. Kansasii immune reconstitution pneumonia • Mycobacterium Avium Complex (MAC) • Cryptococcal Fungemia, meningitis • Histoplasmosis • PML
Effect of HAART on Opportunistic Infection Incidence • Most OI’s have declined 80-90% • OI’s seen now mostly in 3 groups • undiagnosed HIV+ • not in care or not adhering to therapy • long time “battle-scarred warriors” failing after a long history of multiple regimens
Strata of Pyramid • >350 T Cells • 350-200 • 50-200 • <50
>350 T Cells • Increased incidence of diseases that also affect normal hosts: • Recurrent Vaginal Candidiasis • Pulmonary Tuberculosis • Pnuemococcal Pneumonia • Cervical Dysplasia
200-350 T Cells: • Herpes Simplex • Herpes Zoster • Thrush
50-200 T Cells: • Pneumocystis Carinii Pnuemonia • Toxoplasmosis • Cryptococcus
<50 T Cells • CMV Retinitis • Mycobacterium Avium Complex • Cryptosporidiosis • Progressive Multifocal Leukencephalopathy
Ockham's razor does not apply for advanced AIDS • -often multiple diagnoses present simultaneously • ie PCP, CMV, KS, Cocci • 12% of bacterial pneumonias also have PCP • 10% of PCP pneumonia complicated by bacterial infection • search for second etiology if patient not improving
Immune reconstitution diseases(HAART attacks) • MAC adenitis • CMV • TB • PCP
Primary OI prophylaxis • PCP -T cells <200 or thrush • Toxo -T cells <100 and +Toxo titer • MAC - Tcells <50 • TB – INH x 9 months if PPD >5mm or quantiferon-TB positive
Quantiferon vs. TST in HIV patients • Quantiferon not approved for use in immunocomprimised • 147 HIV patients in New Orleans given both tests: • 36% did not return for TST reading • 15 positive by quantiferon • 1 positive by TST • Quantiferon is more sensitive but without a gold standard for latent TB infection cannot say whether it is more or less specific • Another study showed similar positive test result rates but a better correlation with risk factors for quantiferon vs. TST suggesting quantiferon is a more specific test
Quantiferon vs. TST in HIV patients • “Given the high risk for progression to active disease in HIV-infected persons, any HIV-infected person with reactivity on any of the current LTBI diagnostic tests should be considered infected with M. tuberculosis” • ----CDC guidelines, 3/24/09
PCP Prophylaxis • Septra SS or DS qd or DS TIW • Single strength has similar efficacy with fewer adverse reactions (I.e. late onset rash, hepatotoxicity, fever) • 25-50% of AIDS pts. D/c Septra DS due to reactions • Septra Desensitization: • 1cc qd x 3d, then 2cc qd x 3d, then 5ccqd x 3d, then one SS tab qd • Dapsone 100mg qd +pyramethamine 50mg qweek + leukovorin 25mg qweek • Aerosolized pentamadine 300mg q month • Atavaquone 1500mg qd
Toxo prophylaxis • Septra SS or DS qd or DS TIW • Septra Desensitisation: • 1cc qd x 3d, then 2cc qd x 3d, then 5ccqd x 3d, then one SS tab qd • Dapsone 100mg qd +pyramethamine 50mg qweek + leukovorin 25mg qweek • Atovaquone 1500mg qd
MAC prophylaxis • Zithromax 600mg x 2 tabs qweek reduces infection rate 59% • Also seems to reduce risk of PCP
Case Study: HW • 51 yo male with poor adherence to meds • HIV + since at least 1996 • 1st episode thrush March,2005 • C/o dry mouth • Exam: white patches on buccal mucosa • T Cells 54 • Treated with fluconazole, sx resolve
Case Study: HW • Recurrent thrush July, 2005 • Fluconazole again prescribed • September, 2005 • C/o odynophagia • Dx: probably esophageal candidiasis • Fluconazole again prescribed • Sx resolve in 3 days
Case Study: HW • Recurrent odynophagia January, 2006 • Switched to itraconazole liquid • 3 weeks later: • odynophagia resolved • Thrush persists, resolved on re-exam March, 2006 • August, 2006-March, 2007 • Recurrent episodes of thrush and esophageal candidiasis due to non-adherence to intraconazole • Each episode improves when patient is adherent
Case Study: HW • April, 2007 • Persistent thrush despite stated adherence • Switched to Voriconazole • Sx resolve November, 2007 T Cells 5 Weight 121# (baseline 198#) -recurrent odynophagia despite adherence to voriconazole Admitted for IV Capsofungin Sx markedly improve in 24 hours Fungal Cx: Candida Albicans Sensitivities: resistant to fluconazole, itraconazole and voriconazole
Case Study: HW • December 2007-August 2008 • Persistent extensive thrush • Continued on Voriconazole • T cells 54 -> 12 August 2008: moves in with sisters after hospital stay, adherence improves markedly January 2009: T cells 77, thrush much improved April, 2009: T cells 239, thrush resolved
Candida • Thrush • Angular Chelitis • Vaginal Candidiasis • Esophageal Candidiasis
Thrush • cottage cheese plaques • soft palate, buccal mucosa, tonsils • can be removed with a tongue blade • also erythematous form without exudate
Angular chelitis • pain • fissures • erythema • difficulty opening mouth
Recurrent Vaginal Candidiasis • less frequent than you would expect, unless T Cells<100 • can use Fluconazole 200mg qweek for suppression
Esophageal Candidiasis • odynophagia • usually also has thrush (positive predictive value is 90%, but 18% of esophageal candidiasis presents without thrush) • Treat empirically x 5-7 days • if not better, scope to r/o other causes: • CMV, HSV, idopathic esophageal ulcers, lymphoma • Secondary prophylaxis needed
Treatment: • Fluconazole 100-200mg qd until sx resolve • Alternatives for resistant Candida: • Higher dose fluconazole (400-800 mg/d • Itraconazole • Voriconazole • IV Capsofungin • IV Amphotericin
PCP - Who gets it: • Septra prophylaxis highly efficatious • Risk if T Cells <200 or thrush
PCP - Symptoms • insidious onset • 2-4 weeks of progressive symptoms • Fever, sweats, weight loss, fatigue, nonproductive cough • progressive dyspnea • retrosternal discomfort
PCP - Signs • Lung exam usually normal • CXR: bilateral diffuse interstitial infiltrate in 80-90% • LDH>400 in 62% • PO2<75 in 66%
PCP - Diagnosis • Induced sputum x 3 in early AM (all on same day): 50-70% sensitive • Bronchoscopy (+/-Bx): 80-90% sensitive • PCR based tests • To collect sputums or go directly to bronch?
PCP - Treatment • Can begin before Dx confirmed without affecting diagnostic yield • Prednisone 40mg BID x 5d. Then taper over total 21d. • Septra 15mgTMP/kg/d IV div. Q8h x 21d. • Switch to po when improved • give first dose prednisone 15-30 minutes before Septra
Approach to HIV patient with Pneumonia • What is the T Cell Count?