Download
1 / 36
360 likes | 584 Views
2015 -1 0 -27. D E P A R T M E N T OF PE D I A T RI C H E M A T O L O G Y A N D O NC O L O G Y C O LL E GI U M M E D I CU M U M K BY D G O S Z C Z SOLID TUMO R S SE M INAR 5TH Y E A R P R O F . J A N S T Y C Z YŃS K I.

E N D
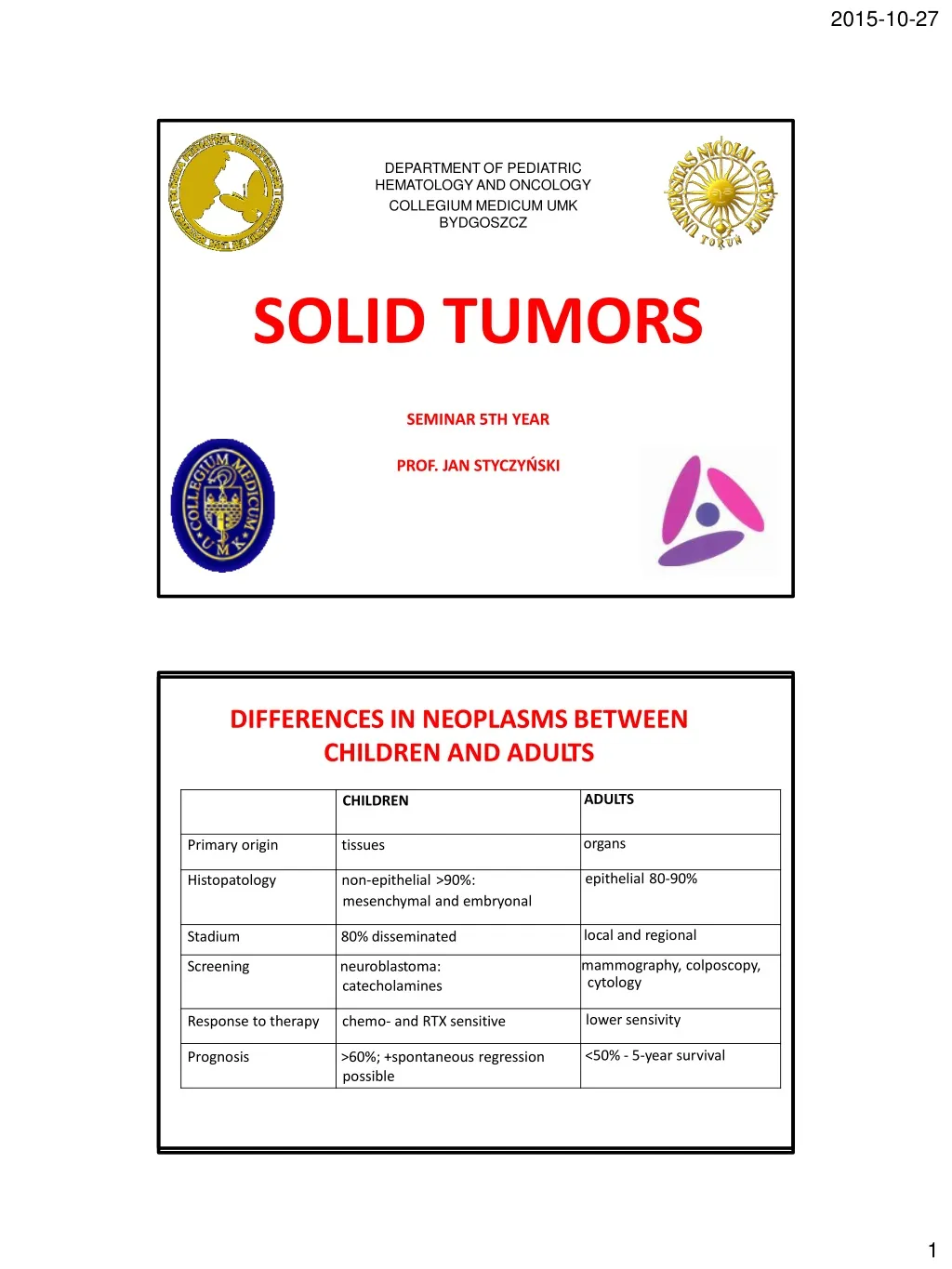
2015-10-27 DEPARTMENTOF PEDIATRIC HEMATOLOGYANDONCOLOGY COLLEGIUMMEDICUM UMK BYDGOSZCZ SOLIDTUMORS SEMINAR5THYEAR PROF.JAN STYCZYŃSKI DIFFERENCESIN NEOPLASMSBETWEEN CHILDRENANDADULTS CHILDREN ADULTS Primary origin tissues organs Histopatology non-epithelial>90%: epithelial80-90% mesenchymalandembryonal Stadium 80%disseminated local andregional Screening neuroblastoma: mammography,colposcopy, Responsetotherapy chemo- andRTXsensitive lower sensivity Prognosis >60%;+spontaneousregression <50%-5-yearsurvival possible catecholamines cytology 1
2015-10-27 AGE-DEPENDENCE • 1y:neuroblastoma,retinoblastoma,hepatoblastoma,Wilmstu • >80%neuroblastomain first3years oflife • 80%Wilmstumorin first 5yearsof life • 2-5y:ALL • 6-10y:braintumors • adolescents– HD,osteosarcoma,Ewingsarcoma,STS • 70%bonetumorsat age>15y • Earlychildhoodand15-18y–gonadal germinaltumorsin boys • At puberty–gonadal germinaltumorsingirls SOLIDTUMORSINCHILDREN • Brain tumors • Sympatheticsystemtumors:neuroblastoma • Nephroblastoma(Wilmstumor) • Softtissuesarcoma (RMS-rhabdomyosarcoma) • Bonetumors(osteosarcoma,Ewingsarcoma) • Germinaltumors(germinoma) • Livertumors(hepatoblastoma,hepatocarcinoma) • Retinoblastoma • Histiocytosis • Raretumors 3
2015-10-27 BRAINTUMORS Supratentorialtumors (astrocytoma) Supratentorialand centrallinetumors (pharyngioma,glioma, Infratentorial (medulloblastoma, ependymoma) 60% LOCALIZATIONOFPRIMARYCNSTUMORSINCHILDREN germinaltumors) tumors CLASSIFICATION I. NEUROEPITHELIALTUMORS -gliomas:astrocytoma,oligodendroglioma,ependymoma,GBM -tumorsofprimaryneuralcells (neuroblastoma,medulloblastoma/PNET) II. PERIPHERALNERVESTUMORS III. MENINGEAL TUMORS IV. LYMPHOMAS V. GERMCELLTUMORS VI. TUMORS OF THESELLAR REGION VII.METASTATICTUMORS 5
2015-10-27 SYMPTOMSANDSIGNS 1.Dysfunction(relatedtolocalizationoftumor) • seizures,paresis(hemiparesis, facialparesis),aphasia,dysphagia, ataxia,dizziness;motor/sensory /visualimpairment,etc 2.Consequencesof intracranialhypertension • headaches,vomiting(earlymorning),nausea,alteredstateof consciousness(somnolence, coma),anisocoria,in infants: elevatedintracranialpressuremaycausean increasein the diameterof theskullandbulgingof thefontanelles BRAIN TUMORDIAGNOSTICS • Imaging: CT, MRI,(PET) • Ophthalmologicalexamination • Biopsyandhisto-pathologicalexamination • CNSfluidexamination • Cancer markers(AFP,HCG) • Endocrinologialexamination • Psychologicalexamination 6
2015-10-27 THERAPEUTICSTRATEGY Strategyis dependent on: • Tumorhistology • Extentofsurgical treatment • Ageofpatient Strategyof management inMB/PNET: • Diagnostics • Surgery • Staging • Post-operativechemotherapy • Radiotherapy • Maintenance chemotherapy NEUROBLASTOMA 8
2015-10-27 NEUROBLASTOMA • Originatesfromimmaturecellsof peripheralsympatheticsystem • 90%diagnosedbefore ageof5 yrs • In90%hormonallyactive (A,NA, DA,VMA) • Other markers: NSE,feritin,LDH NEUROBLASTOMA 9
2015-10-27 NEUROBLASTOMA:SYMPTOMS ANDSIGNS General:Fatigue,loss of appetite, fever,weakness, bone pain, hypertension,anemia Metastases: skull bones,bruising and swelling around theeyesor orbits, swallenbelly, breathingproblemsetc NEUROBLASTOMA Symptomsandsignsrelatedtoprimarysite: ABDOMEN:pain,dyspepticsymptoms, constipation,diarhhoea,swallenbelly,ileus, inferiorvenacavasyndrome CHEST:cough,URTI,chestpain,dyspnea,other breathingproblems,Hornersyndrome, superiorvenacavasyndrome SPINALCORD:weakness,inabilitytostand, crawl,orwalk;myelopathy,pain(radiculitis- like),numbness,paresis,sphincter dysfunctions 10
2015-10-27 NEUROBLASTOMA:DIAGNOSTICS • Imaging(RTG,USG,CT,MRI) • Scintigraphy(localmetabolicactivity:specificmarkerMIBG- metyl-jodo-benzyl-guanidine) • Tissuespecimen:histopathology,immunohistochemistry, cytogenetics,moleculartests • Catecholamines(24-hoururinaryoutput) • Biochemicalmarkers:ferritin,NSE,LDH • Bonemarrowbiopsyandaspiration SCINTIGRAPHYMIBG • Diagnostics • Monitoringoftherapy • Diagnosticsofrelapsein neuro-endocrine system 11
2015-10-27 NEUROBLASTOMA:TREATMENT DIAGNOSTICANDTHERAPEUTICSTRATEGY • Diagnostics-chemotherapysurgerychemotherapy stemcelltransplantationradiotherapyimmunotherapy ADVERSEPROGNOSTICFACTORS • AmplificationofoncogeneN-MYC>10copies • Deletion1p,lackof expressionCD44,TRKA,p75 • Ageover1year • Advancedstage • Boneandbonemarrowmetastases • IncreasedvaluesofNSE,feritin,LDH WILMSTUMOR (NEPHROBLASTOMA) 14
2015-10-27 WILMSTUMOR:CHARACTERISTICS • Originatesfromlowdifferentiatedrenalblastema • Peakincidence:3-4 yearof life • 6%ofallchildhoodneoplasms • Themost frequent kidneytumorinchildren • Secondmostfrequentretroperitonealtumorin children • In1%-familyoccurence • Possibleco-existencewithcongenitaldefects GENETICSYNDROMES CONCOMITANTWILMSTUMOR 7,9%-hamartomas,angiomas,melanocytic naevi 4,4%-congenitaldisordersof urinarytract 2,9%-congenitalhemihypertrophy 2,9%-congenitaldefectsof bones and muscles 1,1%-congenitalaniridia 15
2015-10-27 WILMSTUMOR:SYMPTOMSAND SIGNS 1. generalsymptoms 2.recurrenturinarytract infections 3.erythrocyturia,hematuria 4.hypertension 5.abdominal pain 6.intestinalsymptoms(abdominalswelling,constipation, cramping, darkstools,nausea,vomiting) 7.symptomsofabdominaltumor WILMSTUMOR:DIAGNOSTICS 1.Patienthistory 2.Physicalexamination 3.Urinetests 4.Imaging(USG,CT,RTG) 5.Biochemicaltests 6.Cytogenetictests (del11p) 7.Arteriographyof renal arteries (stadium5) 8.Bonescintigraphy 16
2015-10-27 TREATMENTSTRATEGY pre-operativechemotherapy4-6 weeks nephrectomy (delayed,exceptinfants at stageIorII) post-operativechemotherapy–withrespectto staging radiotherapy(stageIIN+or higher) long-termfollow-up STAGING Staging–atdiagnosis Surgeryandpathologystaging -duringsurgicaloperationandafterhisto-pathologicalexamination I–Tumorislimitedtothekidneyandiscompletelyexcised II–Tumorextendsbeyondthekidneybutiscompletelyexcised III–Unresectableprimarytumor/Lymphnodemetastasis/Tumorispresentat surgicalmargins/Tumorspillageinvolvingperitonealsurfaceseitherbeforeor duringsurgery IV–presenceofhematogenousmetastases(lung,liver, bone,orbrain) V– bilateralrenalinvolvement favorablehistology– lowgrademalignancy intermediatehistology– intermediategrademalignancy unfavorable(anaplastic)histology–highgrademalignancy 17
2015-10-27 SOFTTISSUESARCOMAS RHABDOMYOSARCOMA 19
2015-10-27 CHARACTERISTICS • Tumorsoriginatingfromprimarymesenchymal tissue • Tumorsof muscles,connectivetissueand vessels • Growth by local infiltration– local recurrences • Hematogenousmetastases EPIDEMIOLOGY •6%ofallneoplasmsinchildren •In60%- below5-6yearoflife •Secondpeakofincidence:14-18yrs •In60-70%-rhabdomyosarcoma 20
2015-10-27 HISTOPATHOLOGY Histologicalstructuredeterminesriskstratification and sensitivityto chemotherapy •RMSgroup(RMSembryonal [favorable],alveolar [unfavorable],pleomorphic,anaplastic; extra-bone Ewing sarcoma,sarcomasynoviale) •Non-RMS group (leiomyosarcoma,fibrosarcoma, liposarcoma, angiosarcoma, hemangiopericytoma, lymphangiosarcoma) SYMPTOMSANDSIGNS: DEPENDENTONLOCALIZATION WITHPROGNOSTICVALUE: 1.Head,orbits(perimeningeal localization),neck (40%) 2.Urinarybladder(20%) 3.Abdomen:others(15-20%) 4.Limbs (10%) 5.Others (10%) CLINICALSYMPTOMSANDSIGNS: 1.Presenceof tumor 2.Compressiontoother organs and tissues 21
2015-10-27 DIAGNOSTICS • Patienthistory • Physicalexamination • Imaging ofprimarylocalization:CT /MRI • RTG/scintigraphyof bones • Bonemarrowbiopsy • Biochemicaltest • Other–dependenton localization STAGING • I–localiseddisease,totalresection • II–macroscopictumorresection,microscopic residualtumor • III–partialtumorresection,macroscopicresidual tumor; biopsyonly • IV – metastasespresentatdiagnosis 22
2015-10-27 TREATMENT 1. Inductionchemotherapy–decreasestumormass, decreasesmetastases 2. Local therapy(surgery+ radiotherapy) 3. Adjuvantchemotherapy(supplementary) 24
2015-10-27 BONETUMORS EPIDEMIOLOGY • 5%of allpediatrictumors • Peakincidence:in adolescents(15-19yrs) • Themostfrequent:osteosarcoma • Osteosarcoma–localizedinlongbones(metaphyses) • Ewingsarcoma–localizedinlongbones andflatbones (pelvis) • Metastasestolungs,bones, marrow • In30%patients–metastasesarepresentatdiagnosis 25
2015-10-27 HISTOPATHOLOGY • Osteosarcoma:originatesfrombonecells,localized at bonegrowthcentersinlongbones(metaphyses) • EwingSarcoma:originatesfromneuralcellsin marrow cavity–inlongbones andaxialskeleton • Chondrosarcomaand fibrosarcoma:rareoccurrence 26
2015-10-27 SYMPTOMSAND SIGNS • PAIN–worseatnight • TUMOR–growingrapidly,hard,nopainatexamination • Swelling, restrictedrangeof locomotion,pathologicalfracures • Fever • Paraplegy • In40%of Ewingsarcoma:subfebrile status, anemia, symptomsof infection(infection mask) • Injury(in patientshistory)–indicatesdisease (sickplace) DIAGNOSTICS • Patienthistoryand patient examination • Imaging:RTG/ MRI/CT • Scintigraphyof bones(99TcMDP) • Biochemicaltests(alkalinephosphatase) • ChestCT • Soft tissueinvolvement • Histo-pathology–responsetoinductionchemotherapy 28
2015-10-27 THERAPEUTICSTRATEGY • Pre-operativemulti-agentchemotherapy(aim:decreaseof tumormass,totargetmicro-metastases,to assessthe response tochemotherapy) • Surgery: amputation(endoprosthesis,bonetransplant), therapy ofmetastases • Post-operativechemotherapy • Radiotherapy–onlyin Ewingsarcoma GERMINALTUMORS 30
2015-10-27 GERMINALTUMORS • 6%ofall neoplasmsin children • Originatefromprimarygerminalcells • Localization: •Gonadal(1/3) •Extra-gonadal(2/3) –sacro-coccygalregion,pinealgland, mediastinum,retroperitonealspace • Morefrequent:girls • Peakincidence: –I.Age0-3yrs (mainlyin sacro-coccygalregion) –II.Age>12yrs (mainlyovariantumors) HISTOPATHOLOGY CLASSIFICATION 1.TERATOMA–includesstructuresof3germ layers. In80% - sacro-coccygeallocalization,10%- necklocalization. 2.GERMINOMA–originatesfromprimaryovocyte (dysgerminoma)orseminal cell (seminoma).Localization: gonads, mediastinum,skull.Rarelyin children. 3.CARCINOMAEMBRYONALE 4.YOLKSACTUMOR– themostfrequentgerm celltumor, resembles structuresof primaryyolksack, producesAFP. 5.CHORIOCARCINOMA- rare,malignant,produes-HCG 6.POLYEMBRYOMA– veryrare 7.GONADOBLASTOMA 31
2015-10-27 GERMINALTUMORS:SYMPTOMSANDSIGNS • Abdominaltumor,abdominalpain • Tumorinbuttocksarea • Problemswithdefecation/constipation • Dysuria/ urineretension • Swellingoftestis • Precociouspuberty • Secondaryamenorrhea • Headaches,vomiting,localneurological symptoms • Paininthechest, cough,dyspnea • Legweakness • Congenital abnormalities DIAGNOSTICS • Patienthistory • Patientexamination • Biochemicalandgenetictests • Neoplasticmarkers: AFP,beta-HCG • Imaging ofprimarytumor site • Imaging forpossiblemetastases(bones,chest) 32
2015-10-27 THERAPEUTICSTRATEGY DEPENDS ON: • Initialclinicalstageandpost-operativestage (TNM) • Secretingcharacterof tumor,histology,initialAFP concentration(<or>15 000mg/ml) Twoprognosticgroups: - Standardrisk - High risk THERAPEUTIC STRATEGYINTHERAPYOF MALIGNANTnon- SEMINOMAGERMINALTUMORS(TGMnS) AFP<15 000ng/ml TGMnS histopathology nometa AFP>15 000ng/ml and/ormeta HIGHRISK Carcinoma embryonale TGMnS histopathology non-secreting obligatory Teratomalow-differentiated STANDARDRISK secreting not obligatory 33
2015-10-27 GERMINALTUMORS:TREATMENT • Surgical –solely,onlyinnon-malignantteratoma • Chemotherapy–in mostcases(dependenton stage of surgicalresectionand histology) • Radiotherapy: dysgerminoma- sensitive,ovarian endodermalsinus tumor–lowsensitivity 34
2015-10-27 LIVERTUMORS LIVERTUMORS • hepatoblastoma • hepatocarcinoma • mesenchymoma 1%ofallneoplasmsinchildren Peak incidence:hepatoblastoma-1yr;hepatocarcinoma–12yrs • Liver metastases: – neuroblastoma – Wilmstumor – lymphoma – Langerhanscellhistiocytosis(LCH) • Non-malignanttumors: – hamartoma,nodularhyperplasia,cysts,adenomas,etc 35
2015-10-27 PATHOGENESISOFLIVERTUMORS HBL • Geneticfactors • coexistanceHBLandcongenitalabnormaliies(Beckwith-Wiedeman syndrome,WAGR,neurofibromatosis) • AbnormalitiesofcellularDNAcontent;chromosome11;trisomy20 • Environmentalfactors • Useofsomedrugs(gonadotropinsoranticonceptives);expositionto chemicals;alcoholabuse HCC • HepatitisBinfection;coexistanceHCCwithtyrosinemia;coexistanceHCC withwithbiliaratresia/fibrosis;drugabuse(anabolics) HISTOPATHOLOGY HBL • Mostoften:uni-focallocalizationinrightlobe,withcapsula • Morphology: 1.Epithelialtype(embryonalorgerminalcells) 2.Mixedtype(epithelial ormesenchymalcells)(osteoid) HCC • Multi-focal • Earlymetastases dolocallymphnodesandlungs(rarelytobones) 36
2015-10-27 SYMPTOMSANDSIGNS • Lossof apetite, weight loss,vomitings,abdominaltumor, hepatomegaly • Thrombocytosis,cystationuria RISKGROUPS: • Lowrisk:tumorwithin3 sectors;limitedtoliver(intra-hepatic) • High risk:tumorpresentwithinall4 liversectors and/orpresentwithinabdominalcavity(extra-hepatic) DIAGNOSTICS • Blood count • Livertests(hepaticenzymes,electrolytes, coagulationtests) • -fetoprotein • Chorionicgonadothropin(-HCG) • AntigenCEA • Imaging(rtg,usg,CT, MRI,angiography,scintigraphy) • HBV,HCV • Biopsy • Searchforextraliver foci (thoraxRTG andCT,bonescintigraphy, marrowbiopsy) 37
2015-10-27 TREATMENT • Pre-operativechemotherapy:responsetotherapy, • Surgery (totalsurgerypossiblein 40-50%) • Post-operativesurgery(assupplementarytherapy) • Radiotherapy–limitedvalue,astherapeuticdoseexceedes tolerantdoseforliver IncreasedAFP serumconcentrationindicatesfor active neoplasticprocess RETINOBLASTOMA 38
2015-10-27 CHARACTERISTICS • 2%of allneoplasms inchildren • Themostfrequentintraocularneoplasminchildren • Highlymalignant • Originatesfromlow-differentiatedretinalcells • Mainlyinchildren1-3 years • Uni-or bilateral,uni-ormultifocalstage, • 2/3 oneeye-ball,1/3both eye-balls(usuallynot simultanously), SYMPTOMSAND SIGNS • Grey/greenreflexin pupilla • Leukocoria–whitepupillaryreflex-evidenceof large tumor • Strabismus • Red eye,intraocularpain(secondaryinfection) 39
2015-10-27 DIAGNOSTICS • Ophthalmoscopy • Ocularutrasound • CT of orbits • Head/ brainNMR • Bonemarrowbiopsy • Biochemicaltests(ferritin,NSE,CEA,AFP) TREATMENT • Dependentonclinicalstage,presenceof metastasesand othersymptoms. • Therapyof intraoculardisease include: 1.surgery 2.radiotherapy 3.cryotherapy Examples:teleradiotherapy,brachytherapy,photocoagulation, cryotherapy,laser 42
2015-10-27 SURGICAL TREATMENT Eye-ballenucleation Indications: 1.Unilateraltumor,involvingwholeeye-ball,withlossofretinalintegrity anddisablingvisionpreservation. 2.Tumorwithextensiontoanteriorchamber 3.Glaucomawithintensivepain,lossofvisionduetoiritis. 4.Tumornotrespondingtolocaltherapy 5.Persistentlossofsightwithintraoculartumor 6.Bilateralstagewithcompletelossofvision CHEMOTHERAPY • Improvesresultsof therapyinpatientswithextraocularRET • Notobligatoryinintraocularstage,butitdecreasestumormass andpossiblemetastases • Obligatoryinrelapseafterenucleation • InpatientswithCNSinvolvement: cranialradiotherapy+ intrathecalchemotherapy 43
2015-10-27 RESULTSOF THERAPY • 5-yearsurvivalin80-90%patientsinunilateral,65-70%in bilateraldisease • Prognosis–dependson clinicalstage,localizationand histology • In30-50%patientsvisionispreserved • Overallsurvival80%inextraocularRET RARETUMORS 44
2015-10-27 HEADAND NECK CANCERS • Noseand pharynx cancer • Esthesioneuroblastoma(olfactoryneuroblastoma) • Thyroidtumors • Oralcancer • Parotidcancers • Laryngealtumors THYROIDTUMORS •PossiblecorrelationwithRTXofneck •MENsyndrome 45
2015-10-27 THORACICTUMORS •Breastcancer •Bronchialcarcinoid •Pleuralcarcionama •Oesophagealcarcinoma •Thymomaandthymuscancer •Cardiactumors •Mesothelioma BREAST CANCER •Non-malignantinmostcases •Incidence:bothboysandgirls –Increased riskin girlsafterHD withRTX –Carcinoma> sarcoma –Mammography to be performedfromageof 25 yrs 46
2015-10-27 ABDOMINALTUMORS • Adrenalcortex tumors • Renaltumor • Stomachcancer • Pancreatictumor • Largeintestine cancer • Carcinoid • Vesical carcinoma • Ovariantumor OTHER RARETUMORSIN CHILDREN • Multipleendocrinalneoplasms • Skin neoplasms: –Melanoma –Basal cellcancer –Squamouscellcancer 47

![[0 1 0]](https://cdn0.slideserve.com/536424/slide1-dt.jpg)