Download
1 / 1
10 likes | 72 Views
Analyzing CR referral trends and factors post-ACS in Canada using GRACE registry data. Highlighting CR benefits and medication patterns.

E N D
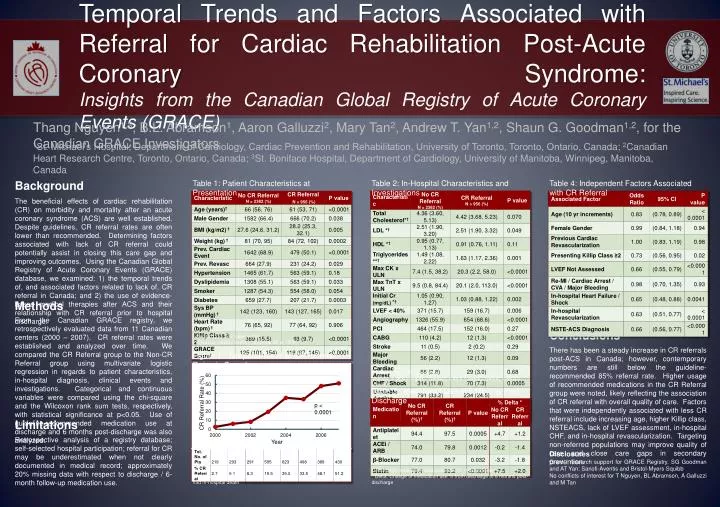
1St. Michael’s Hospital, Department of Cardiology, Cardiac Prevention and Rehabilitation, University of Toronto, Toronto, Ontario, Canada; 2Canadian Heart Research Centre, Toronto, Ontario, Canada; 3St. Boniface Hospital, Department of Cardiology, University of Manitoba, Winnipeg, Manitoba, Canada Temporal Trends and Factors Associated with Referral for Cardiac Rehabilitation Post-Acute Coronary Syndrome: Insights from the Canadian Global Registry of Acute Coronary Events (GRACE) Background Table 1: Patient Characteristics at Presentation Table 2: In-Hospital Characteristics and Investigations Table 4: Independent Factors Associated with CR Referral The beneficial effects of cardiac rehabilitation (CR) on morbidity and mortality after an acute coronary syndrome (ACS) are well established. Despite guidelines, CR referral rates are often lower than recommended. Determining factors associated with lack of CR referral could potentially assist in closing this care gap and improving outcomes. Using the Canadian Global Registry of Acute Coronary Events (GRACE) database, we examined: 1) the temporal trends of, and associated factors related to lack of, CR referral in Canada; and 2) the use of evidence-based medical therapies after ACS and their relationship with CR referral prior to hospital discharge. Thang Nguyen1,3, B.L. Abramson1, Aaron Galluzzi2, Mary Tan2, Andrew T. Yan1,2, Shaun G. Goodman1,2, for the Canadian GRACE Investigators Methods From the Canadian GRACE registry, we retrospectively evaluated data from 11 Canadian centers (2000 – 2007). CR referral rates were established and analyzed over time. We compared the CR Referral group to the Non-CR Referral group using multivariate logistic regression in regards to patient characteristics, in-hospital diagnosis, clinical events and investigations. Categorical and continuous variables were compared using the chi-square and the Wilcoxon rank sum tests, respectively, with statistical significance at p<0.05. Use of guideline-recommended medication use at discharge and 6 months post-discharge was also analyzed. Conclusions † median (25th, 75th) percentile * Previous cardiac event = previous MI or CHF There has been a steady increase in CR referrals post-ACS in Canada; however, contemporary numbers are still below the guideline-recommended 85% referral rate. Higher usage of recommended medications in the CR Referral group were noted, likely reflecting the association of CR referral with overall quality of care. Factors that were independently associated with less CR referral include increasing age, higher Killip class, NSTEACS, lack of LVEF assessment, in-hospital CHF, and in-hospital revascularization. Targeting non-referred populations may improve quality of care and close care gaps in secondary prevention. Figure 1: Temporal Trend of CR Referral Rates in Canada † median (25th, 75th) percentile *mmol/L x 38.6 = mg/dL; **mmol/L x 88.5 = mg/dL; ^mg/dLx 88.4 = μmol/L Table 3: Medication Use at 6 Months Post-Discharge p < 0.0001 Limitations Retrospective analysis of a registry database; self-selected hospital participation; referral for CR may be underestimated when not clearly documented in medical record; approximately 20% missing data with respect to discharge / 6-month follow-up medication use. Disclosures Grant / research support for GRACE Registry, SG Goodman and AT Yan: Sanofi-Aventis and Bristol-Myers Squibb No conflicts of interest for T Nguyen, BL Abramson, A Galluzzi and M Tan † Discharge medication data available for 1950 patients * Delta: Change of medication use % from discharge to 6 months post-discharge *Total Number of Patients = All patients with ACS minus patients who had in-hospital death






















