Download
1 / 41
510 likes | 1.22k Views
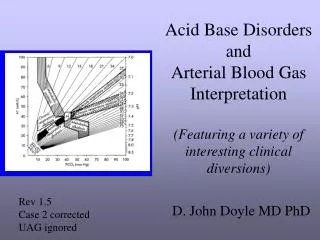
ACE THE ACID – BASE DISORDERS . Cynthia Jackson, RN, MSN. Learning Outcomes. Identify normal ABG values Identify causes and manifestations of acid-base imbalance Analyze ABG values to determine type of acid-base imbalance Develop nursing interventions to manage acid-base imbalance

E N D
ACE THE ACID – BASE DISORDERS Cynthia Jackson, RN, MSN
Learning Outcomes • Identify normal ABG values • Identify causes and manifestations of acid-base imbalance • Analyze ABG values to determine type of acid-base imbalance • Develop nursing interventions to manage acid-base imbalance • Interpret assessment data and ABG values • Apply given ABG values to develop nursing diagnosis and plan nursing care
Three Chemical Buffer Systems • Bicarbonate-Buffer system • Body’s primary buffer system • Kidneys assist by regulating production of bicarbonate (HCO3¯) • Lungs assist by regulating production carbonic acid (H2CO3)
Chemical Buffers • Phosphate-Buffer system: • Phosphate buffers react with either acids or bases to form compounds that slightly alter pH, which provides effective buffering
Chemical Buffers • Protein Buffers • The most plentiful buffers in the body • Work inside and outside the cells • Made up of hemoglobin and other proteins • Protein buffers bind with acids and bases to neutralize them The 3 chemical buffer systems work together to maintain homeostasis—optimal acid-base balance.
BUFFER SYSTEMS Bicarbonate-Carbonic Acid Buffer System C02 + H2O = H2CO3 = H+ + HCO3 Lungs Kidneys
BUFFER SYSTEMS • Bicarbonate-Carbonic Acid Buffer System • Lungs: • Control CO2 and H2CO3 content in ECF. • Regulate by adjusting ventilations based on levels of CO2 in the blood • If CO2 levels are elevated, then increased respiratory rate to eliminate excess CO2--hyperventilation • If CO2 levels are reduced, then the lungs decrease respiratory rate to retain CO2--hypoventilation • Slower response--within 15 minutes
BUFFER SYSTEMS • Bicarbonate-Carbonic Acid Buffer System • Kidneys: • Regulate HCO3¯ in ECF • In acidosis, the kidneys excrete hydrogen ions and conserve bicarbonate ions to restore balance • In alkalosis, kidneys retain hydrogen ions and excrete bicarbonate ions to restore balance • Very slow response--hours to days • The most effective of the buffer systems
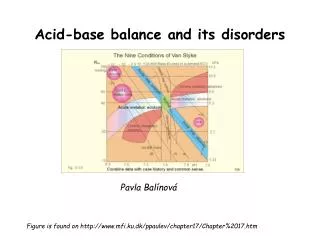
pH 6.8 7.35 7.45 8.0 The normal ration of bicarbonate to carbonic acid is 20:1. As long as this ratio is maintained, the pH remains within the normal range of 7.35 to 7.45. 20 parts bicarbonate (HCOз¯) 1 part Carbonic acid (H2COз)
NORMAL VALUES OF ABGs • pH 7.35 – 7.45 • PaCO2 35 – 45 • HCO3¯ 22 – 26 • PaO2 80 – 100 • SaO2 95 – 100% • BE/BD -2 – +2 Normal pH is slightly alkaline at 7.35 – 7.45
ACIDOSIS • Acidosis is pH < 7.35 • Acidosis occurs when: • Acids (hydrogen ions) accumulate; or • Bases (HCO3) are lost
ALKALOSIS • Alkalosis is pH > 7.45 • Alkalosis occurs when: • Bases (HCO3) accumulate; or • Acids (hydrogen ions) are lost
Partial Pressure of CO2PaCO2 • Reflects the concentration of CO2 in arterial blood • Indicates effectiveness of ventilation • normal range—35-45 • PaCO2 < 35 = alkalosis • PaCO2 > 45 = acidosis
BICARBONATE (HCO3¯) • Normal range is 22 - 26 • HCO3¯ < 22 = acidosis • HCO3¯ > 26 = alkalosis
RESPIRATORY ACIDOSIS • Carbonic acid excess • pH < 7.35 • PaCO2 > 45 • Think SEE SAW; pH goes in opposite direction from PaCO2 • To determine whether compensated or uncompensated look at: • HCO3 normal if uncompensated • pH normal if compensated
Respiratory Acidosis pH 6.8 7.35 7.45 8.0 2 part Carbonic acid (H2COз) 20 parts bicarbonate (HCOз¯)
CAUSES OFRESPIRATORY ACIDOSIS Causes: ALWAYS DUE TO HYPOVENTILATION • Acute Respiratory Acidosis • Acute respiratory conditions (pulmonary edema, pneumonia, acute asthma) • Opiate overdose • Foreign body aspiration • Chest trauma • Chronic Respiratory Acidosis • Chronic respiratory conditions (COPD, cystic fibrosis) • Multiple sclerosis, other neuromuscular diseases, such as Guillain-Barre’, Myasthenia Gravis, Amylotrophic lateral sclerosis • Stroke (CVA)
ADDITIONAL CAUSES OF RESPIRATORY ACIDOSIS Causes: ALWAYS DUE TO HYPOVENTILATION • Severe ARDS • Pneumothorax • Asthma • Chronic bronchitis • Sleep apnea syndrome • Kyphoscoliosis • Extreme obesity • Drugs (anesthetics, narcotics, sedatives, hypnotics) • Mechanical ventilation with low settings causing respiratory acidosis • Cardiac Arrest
MANISFESTATIONS OF RESPIRATORY ACIDOSIS • Acute Respiratory Acidosis • Headache, feeling of fullness in the head • Warm flushed skin, diaphoresis • Blurred vision • Irritability, altered mental status--cloudiness,confusion, disoriented • Decreasing level of consciousness, lethargy, restless, apprehensive • Cardiac arrest, dysrhythmias, tachycardia, hypotension • Chronic Respiratory Acidosis • Weakness • Dull headache • Sleep disturbances with daytime sleepiness • Impaired memory, Personality changes • Bounding pulse with rapid shallow breathing • Cyanosis--late sign
MANAGEMENT OF RESPIRATORY ACIDOSIS • Goal focuses on improving ventilation and ↓ PaCO2 • Pulmonary Hygiene – CPT, coughing, deep breathing, repositioning—semi-fowler’s, suctioning, hyperventilating pt. before and after treatments • Auscultate lungs for CPT effectiveness • Oxygen - Use caution with COPD patient • Monitor resp. rate; may use mechanical ventilation • IVF for hydration & PO fluids--up to 3000ml/24 hours • Medications • Pursed-lip breathing (for chronic resp. acidosis)
RESPIRATORY ALKALOSIS • Carbonic acid deficit • pH > 7.45 • PaCO2 < 35 • HCO3 may be normal in acute stage, but usually decreases in chronic stage • Think SEE SAW: pH increases, PaCO2 decreases (go in opposite direction) • To determine whether compensated or uncompensated look at: • pH normal if compensated • HCO3 normal if uncompensated
Respiratory Alkalosis pH 6.8 7.35 7.45 8.0 20 parts bicarbonate (HCOз¯) 0.6 part Carbonic acid (H2COз)
RESPIRATORY ALKALOSIS CAUSES: ALWAYS DUE TO HYPERVENTILATION • Extreme anxiety-induced hyperventilation (e.g., anxiety) • Fever • Hyperventilation with mechanical ventilation • Hypoxemia, Hypoxia secondary to high altitudes • Pulmonary embolism, acute asthma, pulmonary disease • Pregnancy, particularly during labor • Pain • Gram neg. bacteremia/sepsis • Hepatic failure (liver failure) • Severe anemia • Metabolic acidosis • Drugs: salicylate intoxication, nicotine, xanthines (aminophylline,etc.)
MANIFESTATIONS OF RESPIRATORY ALKALOSIS • Dizziness, lightheadedness • Numbness and tingling (mouth, hands & feet) • Palpitations, tachycardia • Deep rapid breathing with dyspnea • *Cardiac dysrhythmias, chest tightness • Anxious, panic, restlessness • Tremors, muscle weakness • *Carpopedal spasms, tetany, twitching • Seizures, loss of consciousness • Tinnitus • *Hyperreflexia • Diaphoresis • Inability to concentrate *Seen with worsening of symptoms
MANAGEMENT OF RESPIRATORY ALKALOSIS • Identify cause, then treat • If Anxiety, teach slow deep breathing or breathing into paper bag, sedative may be needed • If Pain, administer pain meds. • If needs emotionally upset, provide support • Safety measures • Seizure precautions • Administer oxygen if cause is acute
METABOLIC ACIDOSIS • Base bicarbonate deficit • pH < 7.35 • HCO3¯ < 22 • Think ELEVATOR: pH and HCO3¯ go in same direction, DOWN. • To determine whether uncompensated or compensated look at: • pH normal if compensated • PaCO2normal if uncompensated
Metabolic Acidosis pH 6.8 7.35 7.45 8.0 1 part Carbonic acid (H2COз) 18 parts bicarbonate (HCOз¯)
CAUSES OFMETABOLIC ACIDOSIS • ↑Acid production • Lactic Acidosis • Diabetic Ketoacidosis (DKA) • Drug toxicity (Salicylate) • ↓ Acid Excretion • Renal Failure • ↑ Bicarbonate loss • Diarrhea, ileostomy drainage, intestinal fistula • Biliary or pancreatic fistulas • ↑ Chloride • Sodium chloride IV solutions • Renal tubular acidosis • Carbonic anhydrase inhibitors
MANIFESTATIONS OF METABOLIC ACIDOSIS • Anorexia • Nausea and vomiting • Abdominal pain • Weakness, fatigue, general malaise • ↓ levels of consciousness, confusion, drowsiness & lethargy • Dysrhythmias with hyperkalemia • Bradycardia, decreased BP and cardiac output • Warm, flushed skin, peripheral vasodilation • ↑ RR and depth (Kussmaul) (FIRST CLUE) • Dull Headache • Hyperreflexia and ↓ muscle tone • Shock
MANAGEMENT OF METABOLIC ACIDOSIS • Identify cause and treat (as with DKA) • Administer HCO3¯ • Dialysis (hemodialysis or peritoneal) • Monitor I&O and electrolyte balance • Daily weights • Assess skin color and temperature; VS • Assess for dysrhythmias • Fluid replacement • Safety measures
METABOLIC ALKALOSIS • Base bicarbonate excess • pH > 7.45 • HCO3¯ > 26 • Think ELEVATOR; both go UP • To determine whether compensated or uncompensated look at: • pH normal if compensated • PaCO2 elevated if uncompensated
Metabolic Alkalosis pH 6.8 7.35 7.45 8.0 26 parts bicarbonate (HCOз¯) 1 part Carbonic acid (H2COз)
CAUSES OFMETABOLIC ALKALOSIS • ↑ Acid loss or excretion • Most common are vomiting or gastric suction • Hypokalemia • ↑ Bicarbonate • Alkali ingestion (bicarbonate of soda) • Excess bicarbonate administration • Other causes include: thiazide and loop diuretics, overuse of antacids containing HCO3¯, Cystic Fibrosis, excessive use of corticosteroids
MANIFESTATIONS OF METABOLIC ALKALOSIS • Confusion and apathy, ↓ levels of consciousness • Hyperreflexia • Tetany • Dysrythmias • Hypotension/dizziness and hypoxemia • Seizures • Respiratory failure, slow shallow respirations • Tingling of fingers and toes • Cyanosis • Anorexia, nausea and vomiting • Weakness • Muscle twitching • Symptoms of hypocalcemia, which includes low RR, atrial tachycardia, ventricular disturbances, low K+
MANAGEMENT OF METABOLIC ALKALOSIS • Restoring normal fluid volume • Potassium supplement if hypokalemic • Monitor VS, esp. RR • Monitor I&O and electrolyte imbalances • Assess for S&S hypokalemia (muscle weakness, dec. peristalsis, dysrhythmias, dizziness) • Safety measures • Irrigate NG tubes with NS instead of tap water • Stop NG suction, if possible • Seizure precautions • Patient teaching regarding use of medications (steroids, antacids, diuretics)
INTERPRETING ABGs STEPS: 1. Check the pH to determine whether it is acidosis or alkalosis. • Check the PaCO2 to determine if the problem is respiratory. • Check the HCO3¯ . This provides information about the metabolic aspect of acid base disorders. • Check the PaO2 and the SaO2. Normals for PaO2 is 80-100 and SaO2 is 95 - 100%. • Determine whether compensated or uncompensated
SUMMARY • When evaluating ABGs with a pH in the normal range, use 7.40 as the cutoff: • < 7.40 is acidosis; > 7.40 is alkalosis • Use same idea with CO2: • < 40 is alkalosis; > 40 is acidosis
CASE STUDY #1 • Robert Miller is a 70-year-old diabetic who has a long history of not taking his insulin. He has just been admitted to your unit and you receive the following ABG results; pH 7.26, PaCO2 42, HCO3¯17. Plot these numbers on the grid. Acid Normal Alkaline pH PaCO2 HCO3¯ Disorder: Metabolic acidosis
CASE STUDY #2 • A 50 year old female is brought to the EC following an auto accident. She sustained no injuries, but is extremely upset and anxious. She has been breathing rapidly since the accident and now feels faint. Her ABG results are: pH 7.49, PaCO2 30, HCO3¯23. Plot on the grid. Acid Normal Alkaline HCO3¯ pH PaCO2 Disorder: Respiratory Alkalosis
Case Study #3 • A 64-year-old patient who has a long history of COPD. He presents today with a slight fever and complains of dyspnea and coughing up green-colored sputum. His ABG results are: pH 7.26, PaCO2 52, and HCO3¯ 34. Plot on the grid. Acid Normal Alkalosis pH HCO3¯ PaCO2 Disorder: Respiratory acidosis
Web Sites http://www.wisc-online.com/objects/index_tj.asp?objID=NUR4604 http://www.wisc-online.com/objects/index_tj.asp?objid=NUR4904 http://www.studystack.com/menu-6519