Download
1 / 15
150 likes | 290 Views
Shuhainie Nadia Yusof Nurulraini Mohd Ramli. 24-weeks treatment with extended release methylphenidate improves emotional symptoms in adult ADHD. Introduction. What is ADHD? A chronic disorder Begin during early childhood and continues to adolescence

E N D
Shuhainie Nadia Yusof NurulrainiMohdRamli 24-weeks treatment with extended release methylphenidate improves emotional symptoms in adult ADHD
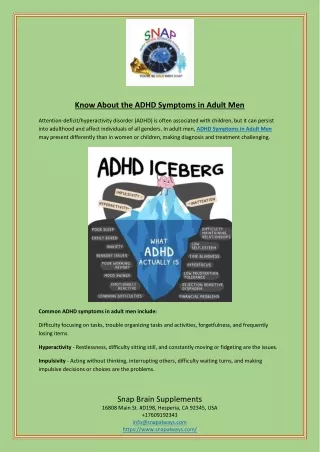
Introduction • What is ADHD? • A chronic disorder • Begin during early childhood and continues to adolescence • Can be full or partial clinical picture in 60% of patients during adulthood
Definition • Major syndromes defines by DSM IV: • Attention disorder • Hyperactivity • Impulsivity • Different concepts was defined by: • CAARS(Conners Adult ADHD Rating Scales, Conners et al. 1999) • BAADS (Brown Adult Attention Disorder Scales, Brown 1996) • Utah criteria of adult ADHD (P. Wender, 1995)
Definition • Hypothesis: co-occuring emotional symptoms accompany those 3 major syndromes can be detected • Inattention, hyperactivity and impulsivity are lifelong and chronic dimension, while others emotional symptoms (eg: poor temper control, affective lability, emotional overreactivity)are episodic phenomena
Medications • 1st line therapy: MPH (methylphenidate) • Altenative drugs: • Amphetamine • Atomoxetine (ATX) in case of non-response to stimulant medication or high abuse potential • Limited knowledge of MPH effect to adult ADHD • Reimherr et al. (2007) : • positive response of MPH • a short 2x4-week not achieve robustness of the treatment over time
Investigation • Objective: • to access the medium- to long-term effects of extended release MPH on emotional symptom and other psychopathology frequently seen in ADHD patients • Subjects: • Outpatients with ADHD aged > 18 years, fulfill DSM-IV criteria for ADHD • Design: • MPH-ER (50% immediate release, 50% extended release)
Study intervention • 1st five weeks: • Flexible dose schedule (10mg/day – 60mg/day) • Lower daily dose if : • Intolerable adverse event • Higher dose not increase improvement • Interval between two doses : 6-8 hours • After 5 weeks: • Min. maintenance dose : 20mg/day
Assessments • General assessments: • Medical history • Physical examination • Vital parameters, etc… • EEG, ECG, complete blood count • Emotional symptoms assessments: • EMS (Emotional Dysregulation Scale) : • 10 items : 0-2 score per item, max score = 20 • ELS (Emotional Lability Scale) : • 6 items : 0-3 score per item, max score = 18 • SCL-90-R (Symptom Checklist 90-Revised)
Result • ITT (intend-to-treat) population: • total: • 363 - 4 (bad data quality/non-compliance) • = 359 patients • MPH ER: 241 patients • placebo: 118 individuals • Drop-out: 110 subjects (lower rate in MPH ER) • MPH ER : 13% adverse effect • Placebo : 25% lack of efficacy • PP (per protocol) population : 249 (183/66)
Discussions • Overall effect sizes of investigation, 0.37 by comparison study by Reimherr et al. (2007), 0.70 • Use of low dose (0.55mg/kg/day) in comparison to Reimherr et al. (0.7mg/kg/day) • Concern of long term safety and tolerability of MPH • To find out whether low doses of MPH ER lead to positive response • Conclusion: differences of effect sizes is a consequence of low dose regimen
Discussions • Improvement of emotional psychopathology (affective lability, temper dyscontrol, and emotional overreactivity) with MPH treatment • Hypothesis : Emotional symptoms are part of ADHD psychopathology rather than comorbid condition • Robust decline of problems with self-concept and of obsessive-compulsive disorder • MPH treatment reduces classical ADHD psychopathology causing also decline of their coping strategy
Discussions • No improvement of anxiety and depression with MPH treatment • Anxiety and depression are only comorbid to ADHD, not part of ADHD emotional psychopathology
Conclusion • Treatment with low doses of MPH-ER in adult patient with ADHD over a period of nearly 6 months leads to a small to medium but robust improvement of emotional symptoms.
Acknowledgements • The World Journal of Biological Psychiatry, 2010; 11: 709-718 • Michael Rosler, Wolfgang Retz, Roland Fischer, Claudia Ose, Barbara Alm, JurgenDeckert, Alexandra Philipsen, Sabine Herpertz& Richard Ammer