Download
1 / 41
420 likes | 887 Views
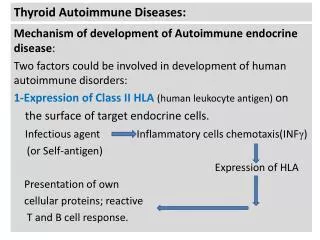
Thyroid diseases. Embryology. 1 st of the body ’ s endocrine glands to develop (28 th day of gestation) Originates as a proliferation of endodermal epithelial cells. As the thyroid start to descent it is still connected to the tongue via thyroglossal duct

E N D
Embryology • 1st of the body’s endocrine glands to develop (28th day of gestation) • Originates as a proliferation of endodermal epithelial cells
As the thyroid start to descent it is still connected to the tongue via thyroglossal duct • This tubular duct later solidifies & obliterates entirely (7-10 wk of gestation) • Some • While the gland descent it passes anterior to hyoid bone & then laryngeal cartilages, forming its mature shape & median isthmus • Completes its descent 7th wk…immediately anterior to trachea
An ectopic thyroid gland • Failure of thyroid to descend→ lingual thyroid • Incomplete descent result in resting point of gland high in the neck or just below the hyoid bone • Imp. Differentiate between ectopic & thyroglossal cyst → total thyroidectomy • Hyoid bone • Sistrunk procedure
If thyroglossal duct does not atrophy → remnant can manifest clinically as thyroglossal cyst, midline mass track anywhere from the thyroid cartilage to base of tongue (rupture) • Pyramidal lobe of thyroid 50%. • Represents a persistence of inferior end of thyroglossal duct that has failed to obliterate
Parafollicular ( C cells), special subset of cells within thyroid gland→ secrete calcitonin • Arise from the ultimobranchial body, which is infiltrated by neural crest cells→ last structure derived from pharyngeal pouches
Anatomy • Under middle layer of deep cervical fascia, thyroid has an inner true capsule → thin & adheres closely to gland • Extension of the capsule →lobes & lobules. Lobules are composed of follicles (structural units of gland) → consist of a layer of simple epithelium enclosing a colloid- filled cavity, which contain iodothyroglobulin (precursor of thyroid hormone) • Epithelial cells: 1) principal (follicular) cells →formation of colloid 2) parafollicular (C) cells →cacitonin
Anterior suspensory ligament extends from superior-medial aspect of each thyroid lobe to cricoid & thyroid cartilage • Posteromedial aspect of gland is attached to side of cricoid cartilage, 1st & 2nd tracheal ring by posterior suspensory (Berry) ligament • This firm attachment to the laryngoskeleton is responsible for its movement during swallowing
Lateral surface of the gland is covered by sternothyroid m. • Sternohyoid & sternothyroid ms. are joined in the midline by avascular fascia that must be incised to retract the muscles laterally to access the gland during thyroidectomy • Should…high in neck cus motor N. supply from ansa cervicalis enters these ms. inferiorly
Arterial spply • Superior & inferior thyroid as. & occasionally thyroid ima a. • Thyroid ima is a single artery which enter the gland from inferior border of isthmus (imp. to consider in tracheostomy→ potential source of bleeding • Superior thyroid a. →1stanterior branch of external carotid a. • Superior to the superior pole the external branch of superior laryngeal N runs with superior thyroid a • High ligation of this artery places the nerve at risk of injury →dysphonia
Inferior thyroid a. → arises from thyrocervical trunk • Closely associated with recurrent laryngeal N, relationship is highly variable
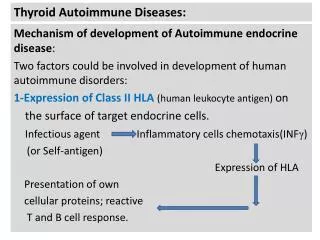
Follicular cellssynthesize & secrete 2 major hormones (T3 & T4) →collectively referred to as thyroid hormone • Thyroid hormone affect all cells within the body except those in brain, spleen, testes & uterus • Regulated through a feedback loop hypothalamus (TRH) ↓ Anterior part of pituitary (TSH) ↓ Thyroid gland (T3 & T4) 90% T4 & 10% T3..in body tissues T4 →T3 greatest metabolic effect
Blood tests • Thyroid Function Test mesure serum TSH free T4&freeT3 • Thyroid Autoantibody estimation. Antithyroid Abthyroid microsomal Ab (TMAb) 95% of patients with Hashimoto.D Thyroglobulin Ab (TGAb) 60% of patients with Hashimoto.D Ab against thyroid TSH receptors (TRAbs) seen in patients with Graves . D • Serum thyrogloublin …used in follow up of metastatic thyroid carcinoma after tyhyroidectomy
X- rays • Plain radiograph chest & thoracic inlet ….to detect retrosternal thyroid extension ,thyroid calcification ,bony or mediastinal LN & lung metastases • CT scan… …For detecting regional &distant metasasis from thyroid cancr • MRI ….diagnosis of cervical LN metastasis
CT scan AP CXR with large retrosternal Goitere
Ultrasound • Used to establish the size & shape of the gland . • May indicate if nodules are single or multiple. • It will distinguish between cystic & solid lesions. (intrathyroid lesion)
Radioisotpe scan • Single or multiple nodules . • Over functioning (hot nodules) or non-functioning (cold nodules) • 20% of cold nodules are malignant • Hot nodules ….rarely malignant Cold n Hot n
How?? • An injected or inhaled or ingested compound labelled with a suitable radionuclide is concentrated in the organ under review . • The emitted radiation is detected by the gamma camera. • Examples of radionuclides… Technetium 99m (99mTc) iodine 131(131I) Krypton (81mKr) Gallium67(67Ga)
FNA • Should be performed in the investigation of all thyroid nodules. • Distinguish between a solid lesion & a cyst • If the lesion is solid….cells are sent for cytological examination • If the lesion is a cyst ….then the fluid can be removed
How?? • A 21 G needle attached to a syringe ,flushed with saline. • is passed several times through the nodule while suction is maintained on the syringe. • The aspirated cells are then smeared onto slide & wet &/or dry fixed. • Results of cytology show benign cells, suspicious cells , malignant cells or the specimen is inadequate & consists of red cells only.
Hypothyroidism • Usually due to autoimmune disorder (Hashimoto thyroiditis). • Investigations.. TSH free T4 &/or T3 Ab : TPO (thyroid peroxidase enzyme) antithyroglobulin
Treatment… thyroxine to render the patient euthyroid normal dose 75-150 ug TSH cheacked every 12-18 months liothyronine(T3) is an alternative elderly patient with ischemic heart disease starting at 25ug & dose every fortnight (to avoid tachyarrhythmias & cardiac failure)
Hyperthyroidism • It may be caused by … Grave’s disease (autoimmune thyrotoxicosis) Toxic multinodular goiter solitary toxic adenoma
Graves’ Disease • Investigations… TSH free T4 &/or T3 90% of patients will have arised TRAb 70% of patients will have arised TPO
Treatment… Initial treatment.. thyroid uptake blocking drugs eg…carbimazole & propylthyouracil SE…neutropenia (sore throat) profuse diarrhea hepatocellular failure B-blockers (propanolol) if the patient is symptomatic with sweating ,termor or tachycardia • Note.. Control of thyrotoxicosis usually takes 6 weeks. But maintenance is required for 18 months
Defenitive treatment.. Radioactive iodine SE: long-term hypothyroidism if inappropriate (young children at home) surgery Sugery previously…subtotal thyroidectomy but…10% recurrent thyrotoxicosis 70% hypothyroidism in long term current surgical tratment of choice….. total thyroidectomy & long term thyroxine postoperatively
Multinodular goitre • Two types.. non-toxic toxic (plummer’s disease) Investigations… TSH (if toxic MNG) FNA…of the dominant nodule if present Ultrasound…may confirm multiple nodules X-ray of thoracic inlet & CT… extent of retrosternal extension & the degree of tracheal deviation & compression .
Treatment… non-toxic goitre ….total thyoidoectomy if there is …rterosternal extension tracheal compression cosmetically unacceptable toxic MNG.. initially…carbimazole then ….total thyroidectomy or radioiodine
Solitary toxic adenoma • Investigations… TSH 99mTcO4 thyroid isotope solitary hot nodule • Treatment.. initially…carbimazole then……thyroid lobectomy or radioactive iodine
Solitary toxic nodule • Investigations… exclude solitary toxic adenoma (TSH) FNA…..to exclude malignancy other investigations (not routinely required for the majority of STNs) ultrasound …discriminate between solid & cysts 99mTcO4 thyroid isotope scan….function of nodule
FNA • Treatment… malignant inadequate suspicious benign Observe Repeat FNA After 6-12months surgery surgery Repeat FNA Thyroid lobectomy
Mangement of thyroid malignancy • Differentiated thyroid carcinoma… which include… papillary thyroid carcinoma follicular thyroid carcinoma • Treatment….according to the Grading system Good prognosis Poor prognosis
Good prognosis • Female < 45yrs old • Male < 40 yrs old • Tumor < 5cm • Minimally invasive follicular carcinoma Treatment • Thyroid lobectomy with subsequent TSH suppression
Poor prognosis • Female > 45 yrs old • Male > 40 yrs old • Tumor >5 cm • Any patient with distant metastsis • Extrathyroidal invasion • Treatment • Total thyroidectomy • subsequent radioiodine (131I) • & TSH suppression with thyroxine
Undifferentiated thyroid carcinoma (anaplastic) Treatment… • Surgery …limited role …… (releive airway obstruction) • External beam radiotherapy &/or chemotherapy (mostly palliative) the vast majority of patients die within 12 months
Medullary thyroid carcinoma Treatment • Total thyroidectomy with central lymph node clearance • Postoperatively …thyroxine replacement (but not TSH suppression) • Postoperative calcitonin measurement is auseful tumor cell marker (follow up)
Thyroid lymphoma • Diagnosed by FNA or trucut biopsy • Should be staged with a bone marrow aspirate & CT scan of chest & abdomen Treatment • If confined to the thyroid alone… thyroid lobectomy with subsequent adjuvant radiotherapy & chemotherapy • Otherwise ….chemoradiation alone
Complication of thyroid surgery • Damage to recurrent laryngeal nerve ….. leading to palsy & causing hoarseness. • Damage to external branch of superior laryngeal nerve … leading to palsy & hoarseness • Hypocalcaemia …caused by damage to parathyroids • Haemorrhage…causing laryngeal oedema & respiratory compromise.