Download
1 / 51
740 likes | 1.91k Views
PHYSEAL INJURY. 2005 년도 소아정형외과학 연수강좌 인제대학교 일산 백병원 주 석규 2005 년 11 월 12 일. ANATOMY. VASCULAR SUPPLY Epiphyseal a.: Supplies proliferative zone chondrocytes Nutrient a. Capillary loops ends at the bone-cartilage interface of the growth plate

E N D
PHYSEAL INJURY 2005년도 소아정형외과학 연수강좌 인제대학교 일산 백병원 주 석규 2005년 11월 12일
ANATOMY • VASCULAR SUPPLY • Epiphyseal a.: • Supplies proliferative zone chondrocytes • Nutrient a. • Capillary loops ends at the bone-cartilage interface of the growth plate • Avascular lower proliferative and hyprtrophic zone
ANATOMY • VASCULAR SUPPLY • Metaphyseal a. and periosteal a. • Collateral supply • Perichondral a. • Supplies perichondral ring of LaCroix
ANATOMY • Cartilagenous Component • Reserve Zone • Proliferative Zone • Hypertrophic Zone
ANATOMY • Cartilagenous Component • Reserve Zone • Chondrocytes produce cartilagenous matrix. • Inactive in cell or matrix turnover • Low oxygen tension lowest calcium content • Not participate in longtitudinal growth
ANATOMY • Cartilagenous Component • Proliferative Zone • Highest oxygen tension • Matrix production and cellular division contribute to longitudinal growth
ANATOMY • Cartilagenous Component • Hypertrophic Zone • Weakest region within the growth plate(low matrix volume, high cellular volume) • Ultimate fate of the hypertrophic zone cell is cell death • Avascular and low oxygen tension • Zone of provisional calcification
Cause of Physeal Injury • Fracture, disuse, radiation, infection, tumor, vascular impairment, neural involvement, metabolic abnormality, frostbite, burns, electric burns, laser injuries, chronic stress, iatrogenic injury
PHYSEAL FRACTURES • History • Fables of Amazon • Hippocrates • Severinus(1632) • Malgaigne(1855) • Poland(1898)
FRCTURE PLANE • -Between calcified and uncalcified cartilage • -Proliferating cells remain with epiphysis. • -The plane is avascular, less bleeding and swelling
Classification • Poland’s Classification(1898):
Classification • Bergenfeldt(1933): First radiologic classification
Classification • Aitken(1936)
Classification • Peterson(1994):
Classifcation • Salter and Harris(1963): • Rang(1969):
Classification • Salter-Harris Classification • Practical, easy to use • Guide to rational treatment • Covers most fractures
Classification • Salter-Harris I: • Complete separation of epiphysis • The Germinal cells remain with the epiphysis • X-ray may seem normal • Shearing, torsion or avulsion injury • Scurvy, rickets, hormonal imbalance, infection • Early healing • Proximal and distal femur
Classification • Salter-Harris II: • Thurston-Holland Fragment • Easy reduction • Over reduction prevented by periosteum • Irreducible; shaft of the bone trapped in the buttonhole tear of periosteum
Classification • Salter-Harris III: • M/C in partially closed physis • Often requires open reduction
Classification • Salter-Harris IV: • Lateral condyle fx, med malleolar fx. • Neglected: loss of position, nonunion, • growth arrest • Not all type IV injuries are the same
Classification • SALTER-HARRIS V: • Crushing injury vs there is no fracture • X-ray at the time of injury shows no abnormality • Can longitudinal force compress the physis enough to kill cells without causing any fracture? • Possibility of disuse or arterial insufficiency • In association with long bone fracture
Classification • SALTER-HARRIS VI: • Peichondral ring injury • Lawn mower injury • Skin loss, difficult skin coverage • Often growth arrest
EPIDEMIOLOGY • Male:Female=2:1 • Boys 14yrs old, girls 11 to 12 yrs old most • common • Phalanges of fingers > distal radius • Distal > Proximal
EVALUATION • 2 Plane radiograph • Stress view • Tomogram • Arthrograms • CT scans • MRI • Ultra Sound
TREATMENT • Gentle reduction • Never forceful repeated reduction • Reduce as soon as possible
TREATMENT • PetersonType I: • -Least potential damage to physis • -Growth arrest 3.4%
TREATMENT • Salter-Harris I: • Growth arrest : • Type I > type II • Distal femur: frequent growth arrest • Proximal tibia: • Vascular injury
TREATMENT • Salter-Harris II: • Scraping of the physis • Relaxed by anesthesia • Metaphyseal fragment prevents overreduction • Periosteum intact on the metaphyseal fragment side • Periosteum impingement • Open reduction • Intact proliferative layer
TREATMENT • Impinged Periosteum (Gruber, JPO, 2002) • -Intact physis: • Degradation of periosteum • Periostum pushed away • -Ablation of Physeal cartilage: • Dramatic injury, growth arrest
TREATMENT • Salter-Harris III: • Needs anatomic reduction • Epiphysis to epiphysis fixation
CONSIDERATIONS IN TREATMENT • Accurate diagnosis: • CT, MRI, • Stress view, • arthrogram
CONSIDERATIONS IN TREATMENT • Reduce or not to reduce: • 7-10 days?
CONSIDERATIONS IN TREATMENT • OR or CR: • -Malreduction of Type I, II vs III,IV • -Impinged periosteum • Immobilization period:
PROGNOSIS • SEVERITY OF THE INJURY • AGE • TYPE OF FRACTURE
COMPLICATIONS • Sepsis • Overgrowth • Malunion • Delayed or nonunion • Compartment syndrome • AVN: proximal femur • Premature Growth Arrest
PHYSEAL ARREST • Occur at the time of injury, during reduction, or • internal fixation • Study: • Skeletal age • Leg length measurement • Localization of bar; • Tomography, CT, scintigraphy, MRI
PHYSEAL ARREST • MRI • - Preop: for mapping the lesion • -Early postop: to detect incomplete resection • -6mths postop: to detect bridge recurrence, migration and necrosis of the interpositional material
PHYSEAL ARREST • Management • Complete arrest vs partial arrest • Cessation of growth without angular deformity • U/E physis; • 10 cm > no treatment • L/E physis; • Pelvic tilt and spine curvature • Low back pain
PHYSEAL ARREST • Management • Osteotomy • Bar excision • Arrest of remaining physis • Shoe lift • Lengthening, • Contralateral shortening, • Physeal distraction, • Transplantation of epiphysis and physis
PHYSEAL ARREST • Management • Leg length discrepancy; • 2.5 cm > shoe lift • 2.5 cm to 5 cm contralateral shortening • Only for femur • Tibia muscle weakness • 5 cm < lengthening
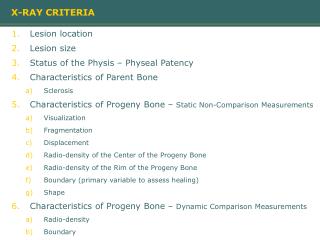
PHYSEAL BAR EXCISION • Physeal bar: • Formed by primary ossification • along areas of vertical septa • Indications of excision: • < 50% of physis involved • > 2 yrs of remaining growth
PHYSEAL BAR EXCISION • Interposition material • To prevent blood from occupying the cavity, organizing, and re-formation of a bone bar • -Bone wax • Autogenous fat: lacks hemostasis function • Cartilage: apophysis of iliac crest • Silicone rubber: commercially not available
PHYSEAL ARREST • BAR EXCISION • Interposition material • Polymethylmethacrylate: load sharing • better for large lesion
PHYSEAL BAR EXCISION • Animal Study • -Cultured chondrocytes • (E.H. Lee) • -Mesenchymal stem cell with TGF beta • (J.I. Ahn)
PHYSEAL ARREST • Classification • Peripheral: approach directly • Elongated: common after S-H IV • Central: approach through metaphysis
PHYSEAL ARREST • Classification • Peripheral: approach directly • Elongated: common after S-H IV • Central: approach through metaphysis
PHYSEAL ARREST • Technique • Burr and dental mirror • Flat and smooth cavity • Do not weaken the epiphysis • Oreo cookie like
PHYSEAL ARREST • Technique • Do not undermine epiphysis and metaphysis • Metal marker • Angular deformity > 20 degrees • Combine with osteotomy
PHYSEAL ARREST • Results • Operated physis may close earlier • Bar 50% < usually fail • Bar 50% < excision should be tried in young children