Download
1 / 41
430 likes | 687 Views
محاضرات م . م سعديه صالح مهدي الزيني كلية الطب البيطري / جامعة الكوفة فــرع الفسلجــة والأدويــة ماجستير أدوية وسموم. Drug affecting the autonomic nervous system.

E N D
محاضرات م.م سعديه صالح مهدي الزينيكلية الطب البيطري / جامعة الكوفة فــرع الفسلجــة والأدويــة ماجستير أدوية وسموم
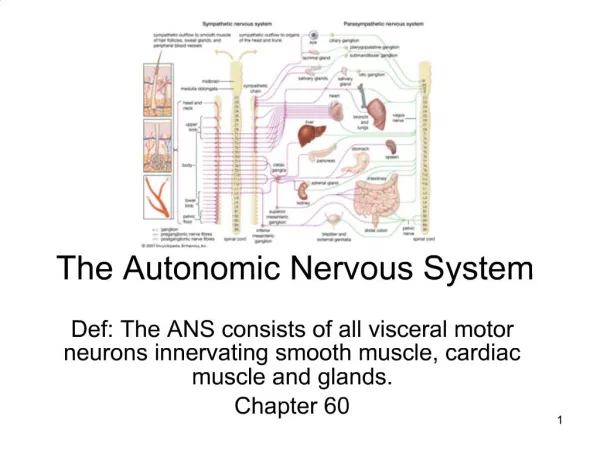
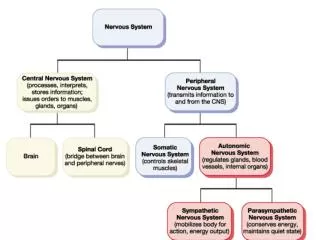
Drugs affecting the autonomic nervous systemDrugs that produce their primary therapeutic effect by altering the function of the autonomic nervous system. These autonomic agents act either by stimulating portions of the ANS or by blocking the action of the ANS. Anatomic of the CNS:
- Efferent fiber the motor portion of the ANS is he major pathway for information transmission from the central nervous system to the involuntary effector tissue (smoth muscle, cardiac muscle and exocrine glands. - Enteric NS is a semiautonomous part of the ANS ,with specific function for the control of the gastrointestinal tract. - Afferent fibers there are sensory fibers,these are of considerable importance for the phsiologic control of the involuntary organs but are directly influenced by only afew drugs 1- 1-spinal roots of origin: The parasympathetic preganglionic motor fibers originate in cranial nerve and sacral segments of the spinal cord. The sympathetic preganglionic fibers originate in the thoracic and lumbar segments of the cord. 2- location of ganglia: most of sympathetic ganglia are located in two paravertebral chains that lie alonge the spinal column. A few located on the anterior of column. Most of parasympathetic ganglia are located in the organs innervated, more distant from the spinal cord 3- length of pre-and postganglionic fiber: The preganglionic sympathetic fibers are short and the postganglionic fibers are long. The opposite is true for the parasympathetic system: the preganglionic parasympathetic fibesr are long and the postganglionic fibers are short. 4-Uninnervated receptors: These include muscarinic receptorson the endothelium of blood vessels,the adrenoceptors on sweat glands and adrenoceptors in blood vessels.
Neurotransmitter aspects of the ANS: • 1-Cholinergic transmission • 2- Adrenergic transmission • Cholinergic transmission: • Acetylcholine:is the primary transmitter in all autonomic ganglia and at the • parasympathetic postganglionic neuron-effecrs cell synapses. • - Synthesis and storage: • Synthesized from acetyl-CoA and cholin by the enzyme choline acetyltansferase. • this transport can be inhibited by hemicholinium. this process can be inhibited by • vesamicol. • - Ach storage into vesicles. • Releaseof AChfrom vesicles in the nerve ending requires the entry of calcium • through calcium channels and triggering of interaction between several proteins • associated with the vesicles and the nerve ending membrane. This interaction results in • the fusion of the vescular and nerve ending membranes, the opening of a pore to the • extracellular space, and the release of the stored transmitter. This release can be • blocked by botulinum toxin. In contrast ,the toxin in black widow spider venom • causes all the Ach stored in synaptic vesicles to empty into the synaptic gap. • Termination of action of Ach: the action of acetylcholine is normally terminated by • metabolism to acetate and choline by the enzyme acetylcholinesterase. The products • are not excreted but are recycled in the body. Inhibition of acetylcholinesterase is an • important therapeutic effect of several drugs.
- Binding to the receptor: Ach release from the synaptic vesicles diffuses across the synaptic space, and it binds to either of tow postsynaptic receptors on the target cell or to presynaptic receptors in the membrane of the neuron that released the Ach. Synthesis and release of Ach from cholinergic neuron
Cholinergic receptors: Cholinoceptors are molecules respond to acetylcholine, these divided into classes: 1 - muscarinic receptors: has been found for five (subtypes M1,M2,M3,M4,M5), located on ganglia of the peripheral nervous system and on the surface of the effector organs. M1 found on gastric cell, M2 found on cardiac cell and smooth muscle, M3 found on bladder, exocrine gland and smoth muscle. 2 - nicotinic receptors: (composed of five subunits) are located in the CNS, adrenal medulla, autonomic ganglia and the neuromuscular junction. Direct - action Cholinergic agonists ( parasympathomimetics) Mimic effects of acetycholine by binding directly to cholinoceptors. These may be classified into tow groups: 1 - Choline esters, which include acetylcholine and synthetic esters of choline such as a- Acetylcholine Pharmacologic effects: the action include 1- Decrease in heart rate and cardiac output. 2- Decrease in blood pressure: Ach cause vasodilation and lowering of blood pressure. 3- Smooth muscle: increase salivary secretion and motility of intestinal, urinary and uterine smooth muscle. 4- Eye: Ach stimulating ciliary muscle contraction for near vision and in the constriction of the pupillae sphincter muscle causing miosis.
b- carbachol has both muscarinic as well as nicotinic action, used to treat glaucoma by causing papillary contraction and decrease in intraocular pressure c- Bethanechol directly stimulate muscrinic receptors, causing increased intestinal motility and used to stimulate the atonic bladder in postoperative. 2- Alkaloids a group of naturally occurring such as muscarine, not used thrapeutically but rather important accidental poison. - pilocarpine therapeutic use in glaucoma choice in the emergency lowering of intraocular pressure. Indirect – action cholinergic agonists (anticholinesterases) The indirect- acting cholinomimetic drugs into two major chemical classes 1- Reversible (Carbamic acid ester): Inhibitors of acetylcholinesteras enzyme indirectly provide a cholinergic action by prolonging the lifetime of acetycholine produce endogenously at the cholinergic nerve endings. This accumulation of acetycholine in the synaptic space .these drug can thus provoke a response at all cholinoceptors in the body, including both muscarinic and nicotinic receptors of the ANS as well as at neuromuscular junctions and in the brain. such as physostigmine and neostigmine the drug increase intestinal and bladder motility.
2- Irreversible (phosphoric acid esters): A number of synthetic organophosphate compounds have the capacity to bind to acetylcholinesterase and . The resulte is long-lasting increase in Ach at all sites where it is released. Many of these drugs are extremely toxic. Related compound, such as parathion, are employed as insecticides. -Ecothiophate: actions include generalized cholinergic stimulation, paralysis of motor function causing breathing difficulties and convulsion. used for treatment of glaucoma. Cholinergic antagonists ( anticholinergic drug): Called cholinergic blocker, parasympatholytics. Cholinoceptor antagonists are readily into subclasses: 1-Basis of their spectrum action they block muscarinic and nicotinic receptors 2-Special subgroup, the cholinesterase regenerators, are not receptor blockers but rather are chemical antagonists of organophosphate cholinesterase inhibitors
Chemical antagonists
Antimuscarinic agents (muscarinic antagonists) • muscarinic antagonists can be subdivided according to their selectivity for M1 receptors, only a few receptor-selective antagonists ( pirenzepine, telenzepine). All of the drugs in general are nonselective. These agents block muscarinic receptors causing inhibition of all muscarinic function. Atropine A tertiary amine belladonna alkaliod, has affinity for muscarinic receptors where it binds competitively, preventing acetylcholine from binding to these sites. Atropine acts both centrally and peripherally. Action - Eye: mydriasis (dilation of the pupil) and cycloplegia (inability to focus for near vision) - Gastrointestinal: used an antispasmodic to reduce activity of the GI tract - Urinary system: used to reduce hypermotility states of the urinary blodder and used in enuresis (involuntary voiding urine) among children - Cardiovascular: at low dose decrease cardiac rate, in higher dose of atropine, the M2 receptors on the sinoatrial node blocker, and cardiac rate increase. Blood pressure is unaffected. - Gland: decrease secretion of saliva gland produce a drying effect on the oral mucous membranes ( xerostomia).
Pharmacokinetic: Absorbed from GI, metabolized by the liver and eliminated in the urine. It has half life of about 4 hours Scopolamine: Is another belladonna alkaloid has longer action and more central effect Action : antimotion sickness, block short term memory causes sedation Ipratropium Used in treating asthma in patients who are unable to take adrenergic agonists and chronic obstructive pulmonary disease. Antinicotinic agents (nicotinic antagonists) 1- ganglion blockers: blockers ganglionic specifically act on the nicotinic receptors of both parasympathetic and sympathetic autonomic ganglia. Some also block the ion channels of the autonomic ganglia. used for treatment of hypertension. hexamethonium and mecamylamin used for this disease. 2- neuromuscular blocking drugs: These drugs block cholinergic transmission between motor nerve endings and the nicotinic receptors on the neuromuscular end plate of skeletal muscle, these drugs include agonists (depolarizing) or antagonists (nondepolarizing) of Ach nicotinic receptors at the neuromuscular junction.
1- Nondepolarizing (competitive) blockers These drugs include tubocuarine considered to be the prototype agent in this class, compete with Ach at the nicotinic receptor at the neuromuscular junction without stimulating the receptors, they are called competitive blockers . These agents have increased the safety of anesthesia, because less anesthetic is required to produce muscle relaxation. Mechanism of action: a- At low doses: these drugs intract with the nicotinic receptos to prevent the binding of acetylcholine, prevent depolarization of the muscle cell membrane and inhibit muscular contraction. Their action can be overcome by increase concentration of Ach in the synaptic gap- for example by administration of cholinesterase inhibitors, such as neostigmine. b-At higher doses: nondepolarizing blockers can block ion channels of the end plate. This leads to further weakening of neuromuscular transmission and it reduces the ability of cholinesterase inhibition to reverse.
Action: Not muscles are equally sensitive to blockade by competitive blockers. Small, rapidly contracting muscles of the face and eye are most susceptible and paralyzed first, followed by the fingers, thereafter, the limb, neck and trunk muscles are paralyzed. thin intercostals muscles are affected and lastly the diaphragm muscles are paralyzed Drug interaction: a- Cholinesterase: Drug such as neustigmine ……can overcome the action of nondepolarizing neuromuscular lockers,but with increase dosage, cholinesterase inhibitors can cause a depolarizing block as a result of elevated Ach concentration at the end plate membrane. b- Halogenated hydrocarbon anesthetic: Drugs such as halothane act t o enhance neuromuscular blocker by exerting a stabilizing action at the neuromuscular junction. c- Aminoglycoside antibiotics: Drug such as gentae rmicin or tobramycin inhibit acetycholine Release from cholinergic nerves by competing with calcium ions. d-Calcium- channel blockess: These agents may increase the muscular block of tubocuraine and other competitive blockers as well as depolarizing blockers.
2- Depolarizing agents: Mechanisme of action:The depolarizing neuromuscular blocking drug (succinylcholine) attaches to the nicotinic receptor and acts like acetylcholine to depolarize the junction. The depolarizing agent persists at high concentrations in the synaptic cleft, remaining attached to the receptor for a relatively longer time and providing a constant stimulation of the receptor. Phase-1: The depolarizing agent first causes the opening of the sodium channel associated with the nicotinic receptors, which results in depolarization of the receptor. Phase-2: This leads to transient twitching of the muscle (fasciculation). Continued binding of the depolarizing agent renders receptor incapable of transmitting further implses. With time continuus depolarization gives way to gradual repolarization as the sodium channel closes or is blockd. This causes resistance to depolarization and a flaccid paralysis.
Action: • Succinylcholin initially produces short-lasting muscle fasciculation, followed • within a few minutes by paralysis because this drug is rapidly broken down • by plasma cholinesterase. The drug does not produce a ganglionic block • except at high doses, but it does have weak histamine-releasing action. • Therapeutic uses • Useful when rapid endotracheal intubation is required during the induction of anesthesia and it is also employed during electroconvulsive shock treatment. • Adverse effects: • hyperthermia malignant with halothane (reducing heat production and relaxing • muscle ton) because block release of Ca++ • - apnea paralysis of diaphragm ( deficient in plasma cholinesterase) • - hyperkalemia potassium lost from within cell ( tissue damage ) • Cholinesterase regenerators: • The cholinesrterase regenerators are not receptor antagonists but belong to a Class of chemical antagonists. These molecules contain an oxime group, which has high affinity for the phosphorus atom in organophosphate insecticides lead to exceeds that of the enzyme active site. Used to treat patients exposed to insecticides such as parathion
Adrenergic transmion: Norepinephrine and epinerphrie: Norepinephrine and epinerphrie is the transmitter, the fiber is termed adrenergic. In the sympathetic system, norepinephrine mediates the transmission of nerve impulses from autonomic postganglionic nerves to effector organs. - Synthesis: Tyrosin is transported by a Na+ linked carrier into the axoplasm of the adrenergic neuron, where it is hydroxylated to dihydroxyphenylalanine (DOPA) by tyrosine hydroxylase, this is the rate – limiting step in the formation of norepinephrine. DOPA is then decarboxylated by the enzyme dopadecarboxylase to form dopamine in the cytoplasm of the presynaptic neuron. Drugs that block synthesis eg, metyrosine. - Storsge of norepinephrine in vesicle: Dopamine enter vesicle by an amine transporter systme and is converted to norepinephrine by the enzyme dopamine B-hydroxylase. Norepinephrine protected from degradation in the vesicle. Transport dopamine into the vesicle is inhibited by reserpine. In the adrenal medulla, norepinephrine methylated to yield epinephrine, both of which are stored in chromaffin cells.
Release of norepinephrine: Influx of calciume causes fusion of the vesicle with the cell membrane in a process known as exocytosis. Release is blocked by guonethidine and bretylium. Binding to alpha receptors: Norepinephrine released from the syneptic vesicles diffuses the syneptic space and binds to either postsynaptic receptors on the effector organ or to presyneptic receptor on the nerve ending. Adrenergic receptors use both the cyclic adenosine monophosphate (cAMP) second-messenger system,2 and the phosphatidylinositol cycle,3 to transduce the signal into an effect. Removal of norepinephrine: - diffuse out of the syneptic space and enter the general circulation. - Metabolizes to o-methylated derivations by postsynaptic cell membrane associated catechol o-methyltransferase (COMT) in the syneptic apace. Inactive norepinephrine metabolism are excreted in the urine. - Recaptured by uptake system that pumps the norepinephrine back into the neuron.
Adrenergic receptors: Adrenoceptors are divided into several subtype: 1- Alpha adreoceptorsThese receptors show a weak response to the synthetic agonist isoproterenol, but they are responsive to the to the naturally occurring catecholamines epinephrine and norepinphrine. These are located on, blood platelets, fat cells and neurons in the brain. Alpha receptor are subdivided into two subgroups: a-Alpha-1 receptors: These are present on the postsynaptic membrane of the effector organs and mediate many of the classic effects. Activation of alpha-1 receptors initiates a series of reactions through a G protein activation of phospholipase. These receptors subdivided into alpha-1 A,B,C,D b-Alpha-2 receptors: These are located on presyneptic nerve endings and other cells, such as the B cell of the pancreas and on some vascular smooth muscles cells. When a sympathetic adrenergic nerve is stimulated, the releasednorepinephrine traverses the synaptic cleft and interacts with the alpha-1 receptors. A portion of the releasednorepinephrine (circles back) and reacts with alpha -2 receptors on the neuronal membrane. The stimulation of the alpha-2 receptor causes feedback inhibition of the release of norepinephrine from the stimulated adrenergic neuron. These receptors subdivided into alpha-2 A,B,C,D.
2- Beta receptors: These are receptors, characterized by a strong response to isoproterenol with less sensitivity to epinephrine and norepinephrine. The B-adrenoceptors can be subdivided into three major subgroups, B-1, B-2, and B-3, based on their affinities for adrenergic agonists and antagonists. B-1Receptors have approximately equal affinities for epinephrineand norepinephrine, whereas B-2 receptors have a higher affinity for epinephrinethan for norepinephrine. Thus, tissues with a predominance of B-2 receptors (such as the vasculature of skeletal muscle) are particularly responsive to the hormonal effects of circulating epinephrinereleased by the adrenal medulla. Distribution of receptors:Adrenergically innervated organs and tissues tend to have a predominance of one type of receptor. For example, tissues such as the vasculature to skeletal muscle have both alpha-1 and B-2 receptors, but the B-2 receptors predominate. Characteristic responses mediated by adrenoceptors: It is useful to organize the physiologic responses to adrenergic stimulation according to receptor type, because many drugs preferentially stimulate or block one type of receptor. As ageneralization, stimulation of alpha-1 receptors characteristically produces vasoconstriction (particularly in skin and abdominal viscera) and an increase in total peripheral resistance and blood pressure. Conversely, stimulation of B-1 receptors characteristically causes cardiac stimulation, whereas stimulation of B-2 receptors produces vasodilation (in skeletal vascular beds) and bronchiolar relaxation.
Type Tissue Actions • Alpha-1 Most vascular smooth muscle Contraction • Pupillary dilator muscle Contraction (dilates pupil) • Pilomotor smooth muscle Erects hair • Prostate Contraction • Alpha 2 Adrenergic and cholinergic nerve Inhibition of transmitter • terminals release • Platelets stimulates Aggregatio • Some vascular smooth muscle Contraction • Fat cells Inhibition of lipolysis • Beta -1 Heart Increases force and rate • Beta-2 Respiratory, uterine, and vascular smooth relaxation • muscle Promotes smooth muscle liver (human) stimulate glycogenolysis • pancreatic B cell stimulate insulin release • Beta-3 Fat cells Activates lipolysis Distribution of Adrenoceptor Subtypes.
Mechanism of action of the adrenergic agonists 1- Direct-acting agonists: These drugs act directly on alpha or beta receptors, producing effects similar to those that occur following stimulation of sympathetic nerves or release of the hormone epinephrinefrom the adrenal medulla. Examples of direct-acting agonists include 2- Indirect-acting agonists: These agents, which include amphetamine, cocaine and tyramine, may block the uptake of norepinephrine or are taken up into the presynaptic neuron and cause the release of norepinephrine from the cytoplasmic vesicles of the adrenergic neuron. As with neuronal stimulation, the norepinephrine then traverses the synapse and binds to the alph or beta receptors. 3- Mixed-action agonists: Some agonists, such as ephedrine, pseudoephedrineand metaraminol, have the capacity both to stimulate adrenoceptors directly and to release norepinephrine from the adrenergic neuron.
Direct-Acting Adrenergic Agonists Direct-acting agonists bind to adrenergic receptors without interacting with the presynaptic neuron. As a group, these agents are widely used clinically. Epinephrine Epinephrine is one of four catecholamines - epinephrine, norepinephrine, dopamine, and dobutamine commonly used in therapy. The first three catecholamines occur naturally in the body as neurotransmitters; the latter is a synthetic compound. Epinephrineis synthesized from tyrosine in the adrenal medulla and released, along with small quantities of norepinephrine, into the bloodstream. Epinephrineinteracts with both alpha and beta receptors. At low doses, beta effects (vasodilation) on the vascular system predominate, whereas at high doses, alpha effects (vasoconstriction) are strongest. Actions: -Cardiovascular: The major actions of epinephrine are on the cardiovascular system. Epinephrine strengthens the contractility of the myocardium (positive inotropic: beta-1 action) and increases its rate of contraction (positive chronotropic: beta-1 action). Cardiac output therefore increases. With these effects comes increased oxygen demands on the myocardium. Epinephrineconstricts arterioles in the skin, mucous membranes, and viscera (alpha effects), and it dilates vessels going to the liver and skeletal muscle (beta-2 effects). Renal blood flow is decreased. Therefore, the cumulative effect is an increase in systolic blood pressure, coupled with a slight decrease in diastolic
-Respiratory: Epinephrinecauses powerful bronchodilation by acting directly on bronchial smooth muscle (beta-2 action). This action relieves all known allergic- or histamine-induced bronchoconstriction. Epinephrinerapidly relieves the dyspnea and increases the volume of gases inspired and expired. Epinephrine also inhibits the release of allergy mediators such as histamines from mast cells. -Hyperglycemia: Epinephrinehas a significant hyperglycemic effect because of increased glycogenolysis inthe liver (beta-2 effect), increased release of glucagon (beta-2 effect), and a decreased release of insulin (alpha-2 effect). -Lipolysis: Epinephrine initiates lipolysis through its agonist activity on the beta receptors of adipose tissue. Therapeutic uses -Bronchospasm: Epinephrineis the drug used in the intreatment of acute asthma and anaphylactic shock, epinephrineis the drug of choice; within a few minutes after subcutaneous administration. Selective beta-2 agonists, such as albuterol, are presently favored in the chronic treatment of asthma because of a longer duration of action and minimal cardiac stimulatory effect. -Glaucoma: In ophthalmology, a two-percent epinephrine solution may be used topically to reduce intraocular pressure in open-angle glaucoma. -Anaphylactic shock: Epinephrineis the drug of choice for the treatment of Type I hypersensitivity reactions in response to allergens. -Anesthetics: The effect of the drug is to greatly increase the duration of the local anesthesia.
Pharmacokinetics: Epinephrinehas a brief duration of action (due to rapid degradation). epinephrineis given intravenously, subcutaneously, by endotracheal tube, by inhalation. Oral administration is ineffective, Only metabolites are excreted in the urine. Adverse effects: - CNS disturbances: adverse CNS effects that include anxiety, fear, tension, headache, and tremor. - Hemorrhage: The drug may induce cerebral hemorrhage as a result of a marked elevation of blood pressure. - Cardiac arrhythmias, Pulmonary edema Interactions: - Hyperthyroidism: Epinephrinemay have enhanced cardio-vascular actions in patients with hyperthyroidism. - Cocaine: In the presence of cocaine, epinephrineproduces exaggerated cardiovascular actions. This is due to the ability of cocaine to prevent reuptake of catecholamines into the adrenergic neuron - Diabetes: Epinephrine increases the release of endogenous stores of glucose. In the diabetic, dosages of insulin may have to be increased. - Beta Blockers: These agents prevent epinephrine's effects on b- receptors, leaving alpha-receptor stimulation unopposed. This may lead to an increase in peripheral resistance and an increase in blood pressure. - Inhalation anesthetics: Inhalational anesthetics sensitizethe heart to the effects of epinephrine,which may lead to tachycardia.
Norepinephrine Because norepinephrine is the neuromediator of adrenergic nerves, it should theoretically stimulate all types of adrenergic receptors. In practice, when the drug is given in therapeutic doses to humans, the Alpha- adrenergic receptor is most affected. - Cardiovascular Actions: • Vasoconstriction: Norepinephrine causes a rise in peripheral resistance due to intense vasoconstriction (alpha-1), increase blood pressures. The increase heart rate (inotropic) due to beta-1 stimulation • Therapeutic uses: used to treat shock, because it increases vascular resistance and, therefore, increases blood pressure. It is never used for asthma or in combination with local anesthetics. • Pharmacokinetics: Norepinephrine may be given IV for rapid onset of action. The duration of action is 1 to 2 minutes following the end of the infusion period. It is poorly absorbed after subcutaneous injection and is destroyed in the gut if administered orally. Metabolism is similar to that of epinephrine. • Adverse effects: These are similar to those of epinephrine.
Isoproterenol Isoproterenol is a direct-acting synthetic catecholamine that predominantly stimulates both beta-1 and beta-2 adrenergic receptors. Actions: - Cardiovascular:Isoproterenol produces intense stimulation of the heart to increase its rate and force of contraction, causing increased cardiac output. - Pulmonary: rapid bronchodilation is produced by the drug (beta-2 action). Therapeutic uses: Isoproterenolis now rarely used as a broncho-dilator in asthma. It can be employed to stimulate the heart in emergency situations. Pharmacokinetics:Isoproterenol can be absorbed systemically by the sublingual mucosa Dopamine Dopaminethe immediate metabolic precursor of norepinephrine, activate alpha and beta-adrenergic receptors. - at higher doses (alpha-1 receptors) cause vasoconstriction by activating. - at lower doses, it stimulates beta-1 cardiac receptors. In addition, D1 and D2 receptors occur in the blood vessels mesenteric and renal. - D1causes vasodilation. - D2 receptors are found on presynaptic receptors prevent release norepinephrine. These receptors are not affected by alpha or beta blocking drugs and are found in the autonomic ganglia and in the CNS.
Actions: - Cardiovascular: a stimulatory effect on the beta-1 receptors of the heart, having both inotropic and chronotropic - Renal and visceral:dilatation by activating D1 receptors Therapeutic uses: - Shock: given by continuous infusion. - stimulating heart by beta-1 receptors to increase cardiac output, and alpha- 1 receptors on blood vessels to increase total peripheral resistance. - increased blood flow to the kidney enhances the glomerular filtration rate Adverse effects: nausea, hypertension, arrhythmias. Dobutamine Actions: a synthetic, direct-acting catecholamine that is a beta-1-receptor agonist. It increases cardiac rate and output Therapeutic uses: used to increase cardiac output in congestive heart failure Adverse effects:should be used with caution in atrial fibrillation, because the drug increases atrioventricular conduction. Oxymetazoline is a direct-acting synthetic adrenergic agonist that stimulates both alpha-1 and alpha-2 adrenergic receptors. - used locally in the eye or the nose as a vasoconstrictorand decrease congestion. congestion.
Phenylephrine is a direct-acting, synthetic adrenergic drug that binds to alpha receptors. - Itis a vasoconstrictor that raises blood pressures. It has no effect on the heart itself but cause reflex bradycardia. - used topically on the nasal mucous membranes as decongestant. - used to raise blood pressure in hypotension Methoxamine is a direct-acting, synthetic adrenergic drug that binds to alpha receptors, causing vasoconstriction. its effects on the vagus nerve by reflex increase blood pressure - used clinically to relieve attacks of paroxysmal supraventricular tachycardia. - used to overcome hypotension during surgery involving halothaneanesthetics. Adverse effects include hypertensive headache and vomiting. Clonidine is an alpha-2 agonist that is used in essential hypertension to lower blood pressure because of its action in the CNS . Metaproterenol, Albuterol, pirbuterol, and terbutaline, Salmeterol and formoterol Beta-2 agonist producing little effect on the heart. Itproduces dilation of the bronchioles. The drug is useful as a bronchodilator in the treatment of asthma
Indirect-Acting Adrenergic Agonists Indirect-acting adrenergic agonists cause norepinephrine release from presynaptic terminals or inhibit the uptake of norepinephrine. These agents do not directly affect postsynaptic receptors. Amphetamine The marked central stimulatory action of amphetamine is often mistaken by drug abusers as its only action. the drug can increase blood pressure significantly by alpha-agonist action on the vasculature as well as beta stimulatory effects on the heart. Its peripheral actions are mediated primarily through the blockade of norepinephrine uptake and cellular release of stored catecholamines; thus, amphetamineis an indirect-acting adrenergic drug. It use for treating hyperactivity in children, narcolepsy, and appetite control. Its use in pregnancy should be avoided because of adverse effects on development of the fetus. Tyramine Tyramine is not a clinically useful drug, but it is important because it is found in fermented foods, such as ripe cheese and Chianti wine. It is a normal by product of tyrosine metabolism. Cocaine Cocaine is unique among local anesthetics in having the ability to block the Na+/K+-activated ATPase.
Sites of action of direct-, indirect-, and mixed-acting adrenergic agonists.
Mixed-Action Adrenergic Agonists Mixed-action drugs induce the release of norepinephrine from presynaptic terminals, and they activate adrenergic receptors on the postsynaptic membrane. Ephedrine and pseudoephedrine Ephedrineand and pseudoephedrine are plant alkaloids, that are now made synthetically. These drugs are mixed-action adrenergic agents. They not only release stored norepinephrine from nerve endings but also directly stimulate both alpha and beta receptors. Ephedrine and pseudoephedrineare not catechols and are poor substrates for COMT (catechol O-methyltransferase) and MAO (adenosine monophosphate); thus, these drugs have a long duration of action. Pharmacokinetics: excellent absorption orally and penetrate into the CNS. Ephedrineis eliminated largely unchanged in the urine, and pseudoephedrine incomplete hepatic metabolism before elimination in the urine. Side effect: Ephedrineraises blood pressures by vasoconstriction and cardiac stimulation. Therapeutic uses: - Ephedrine used in chronic treatment of asthma to prevent attacks. - Ephedrine improves motor function in myasthenia gravis.with anticholinesterases. -Ephedrine stimulation ofthe CNS produce increases alertness, decreases fatigue, and prevents sleep and improves athletic performance. -Pseudoephedrineis primarily used to treat nasal and sinus congestion or congestion of theeustachian tubes.
Adrenergic Antagonists(blockers or sympatholytic) The adrenergic antagonists bind to adrenoceptors but do not trigger the usual receptor-mediated intracellular effects. These drugs act by either reversibly or irreversibleattaching to the receptor, thus preventing its activation by endogenous catecholamines. These are classified according to affinities for alpha or beta receptors. Alpha Adrenergic Blocking Agents blockade of these receptors reduces the sympathetic tone of the blood vessels, This induces a reflex tachycardia resulting from the lowered blood pressure. Phenoxybenzamine is nonselective, noncompetitive, irreversible), linking to both alpha-1 postsynaptic and Alpha-2 presynaptic receptors. The actions about 24 hours after a single administration. Actions: a- Cardiovascular effects: By blocking alpha receptors, prevents vasoconstriction. Decrease blood pressure but increase cardiac output by reflex tachycardia due to decreased peripheral resistance, inhibitory alpha- 2 receptors in the heart b- Epinephrine reversal: All alpha adrenergic blockers reverse the alpha agonist actions of epinephrine the vasoconstrictive action of epinephrineis interrupted but vasodilation of other vascular caused by stimulates beta receptors on the heart is not blocked .Therefore, the systemic blood pressure decreases in response to epinephrinegiven in the presence of phenoxybenzamine.
Therapeutic uses: - used in the treatment of pheochromocytoma, before surgery removalto prevent the hypertensive. - effective in treating Raynaud's disease. - Autonomic hyperreflexia . Adverse effects:can cause hypotension, nasal stuffiness, nausea, and vomiting. Phentolamine competitive block of alpha-1 and alpha-2 receptors. The drug's action lasts for 4 hours side effect cause tachycardia, arrhythmias and anginal pain. Used for diagnosis of pheochromocytoma. Prazosin, terazosin, doxazosin, alfuzosin, and tamsulosin are selective competitive blockers of the alpha-1 receptor. The first three drugs are - useful in the treatment of hypertension . -Tamsulosin and alfuzosin are indicated for the treatment of prostatic hyperplasia. -Metabolism leads to inactive products that are excreted in the urine except for those of -doxazosin, which appear in the feces. Doxazosinis the longest acting of these drugs.
- Cardiovascular effects: decrease peripheral vascular resistance and lower arterial blood pressure Therapeutic uses: - hypotensive response that can result in syncope ( first-dose) effect, may be minimized by adjusting the first dose to 1/3 or 1/4 of the normal dose. - Prostatic hypertrophy decreases tone in the smooth muscle of the bladder neck and prostate and improves urine flow. Adverse effects: dizziness, a lack of energy, nasal congestion, headache, drowsiness, and orthostatic Due to retain sodium and fluid used along with a diuretic. Yohimbine is a selective competitive alpha- 2 blocker. It is found as a component of the bark of the yohimbe tree. Uses: as a sexual stimulant andused to relieve vasoconstriction associated with Raynaud's disease.
Beta- Adrenergic Blocking Agents beta blockers are competitive antagonists, divided into nonselective (beta-1 beta- 2 receptors) and cardioselective beta-1 receptors. These drugs also differ in - intrinsic sympathomimetic activity, - CNS effects - pharmacokinetics. Although all beta blockers lower blood pressure in hypertension without postural hypotension, because the alpha adrenoceptors remain functional. Uses: angina, cardiac arrhythmias, myocardial infarction, congestive heart failure, hyperthyroidism, and glaucoma and prophylaxis of migraine (headaches). Propranolol ( ideral ) nonselective beta antagonist, blocks ( beta-1 and beta-2) receptors. Actions: - Cardiovascular: Propranolol diminishes cardiac output, having both negative inotropic and chronotropic effects. It directly depresses sinoatrial and atrioventricular activity, and decreased consumption of oxygen these effects are useful in the treatment of angina - Peripheral vasoconstriction: Blockade of beta receptors prevents beta-2 mediated vasodilation. The reduction in cardiac output leads to decreased blood pressure and reduced blood flow to the periphery.
- Bronchoconstriction: Blocking beta-2 receptors causes contraction of the bronchiolar smooth muscle (asthma). - Increased Na+ retention: Reduced blood pressure causes a decrease in renal perfusion, resulting in an increase in Na+ retention, (combined with a diuretic). - Disturbances in glucose metabolism: beta blockade leads to decreased glycogenolysis ( not to be given in case of insulin-dependent diabetic) - Blocked action of isoproterenol: block the actions of isoproterenol and beta blocker of epinephrinebut norepinephrine Therapeutic effects: - Hypertension: lowers blood pressure in hypertension by Decreased cardiac output and inhibition of renin release from the kidney - Glaucoma: used in chronic treatment (timolol) neither affects the ability of the eye to focus for near vision nor change pupil size, - Migraine: in chronic migraine, the mechanism may depend on the blockade of catecholamine-induced vasodilation in the brain vasculature. - Hyperthyroidism: In acute hyperthyroidism (thyroid storm), prevent cardiac arrhythmias. - Angina pectoris: useful in the chronic management of stable angina, decreases the oxygen requirement of heart muscle and reducing the chest pain - Myocardial infarction: prophylactic use in myocardial infarction reduces infarct size and hastens recovery. The mechanism for these effects may be a blocking of the actions of circulating catecholamines, which would increase the oxygen demand, also reduces the incidence of sudden arrhythmic death after myocardial infarction.
Adverse effects: Bronchoconstriction: asthma. Arrhythmias: Treatment with β-blockers must never be stopped quickly because of the risk of precipitating cardiac arrhythmias, which may be severe. Sexual impairment: Because sexual function in the male occurs through alpha adrenergic activation, beta blockers do not affect normal ejaculation or the internal bladder sphincter function. Drug interactions: Drugs that interfere with the metabolism of propranolol, such as cimetidine, fluoxetine, paroxetine, and ritonavir, may potentiate its antihypertensive effects. Conversely, those that stimulate its metabolism, such as barbiturates, phenytoin, and rifampin, can decrease its effects. Timolol and nadolol: Nonselective beta antagonists Timolol used in chronic glaucoma and occasionally, hypertension. Acebutolol, atenolol, metoprolol, and esmolol: Selective beta-1antagonists - eliminate the unwanted bronchoconstrictor effect (beta-2 effect) in asthma. - Cardioselective beta -1 blockers, at low doses (50-100) times than bera-2 blockers - These drugs lower blood pressure in diabetic hypertensive patients. - Esmolol has a very short lifetime due to metabolism of an ester linkage. It is only given intravenously if required during surgery
Pindolol and acebutolol: Antagonists with partial agonist activity Actions: Cardiovascular: have intrinsic sympathomimetic activity (ISA). These partial agonists stimulate the beta receptor, yet they inhibit stimulation by the more potent catecholamines, epinephrineand norepinephrine. -These are effective in hypertensive patients with moderate bradycardia, because decrease effect on heard rate and cardiac output is less pronounced - Carbohydrate metabolism is less affected (valuable in the treatment of diabetics) - Not used as antiarrhythmic agents Labetalol and carvedilol: Antagonists of both alpha- and betaadrenoceptors Actions: reversible blocke alpha and beta receptors. used in treating the elderly or black hypertensive patients for whom increased peripheral vascular resistance is undesirable. They do not alter serum lipid or blood glucose levels. [Note: In general, black hypertensive patients are not well controlled with β-blockers.] and used in pregnancy-induced hypertension. Adverse effects: Orthostatic hypotension and dizziness
Drugs Affecting Neurotransmitter Release or Uptake They effects indirectly on the adrenergic neuron by causing the release of neurotransmitter from storage vesicles or alter the uptake of the neurotransmitter into the adrenergic nerve. Reserpine Plant alkaloid, blocks the amines transport system Mg2+/adenosine triphosphate (ATP) from the cytoplasm into storage vesicles, has a slow onset, a long duration of action, and effects that persist for many days. Decrease blood pressure. Guanethidine blocks the release of stored norepinephrine as well as displaces norepinephrine from storage vesicles (thus producing a transient increase in blood pressure). Side effect: causes orthostatic hypotension and interferes with male sexual function. Cocaine Although cocaine inhibits norepinephrine uptake, it is an adrenergic agonist.