Download
1 / 1
10 likes | 97 Views
EPILEPSY IS THE MAJOR MANIFESTATION IN THE RING 14 SYNDROME Simona Giovannini, MD1, Daniela Orteschi, PhD2, Giuseppe Gobbi, MD1 , Elvio Della Giustina, MD3, Angela Scarano, MD3, Marcella Zollino, MD2, Giovanni Neri, MD2

E N D
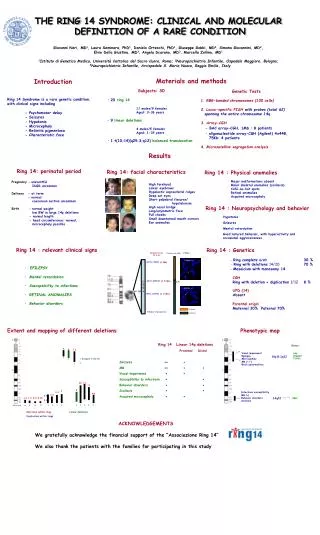
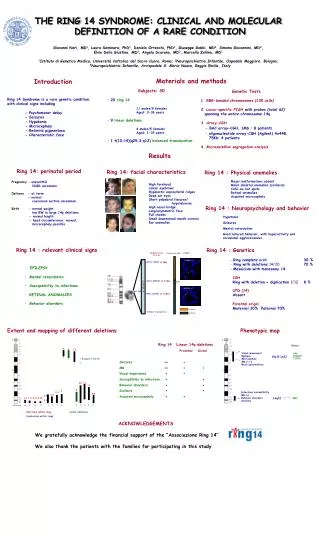
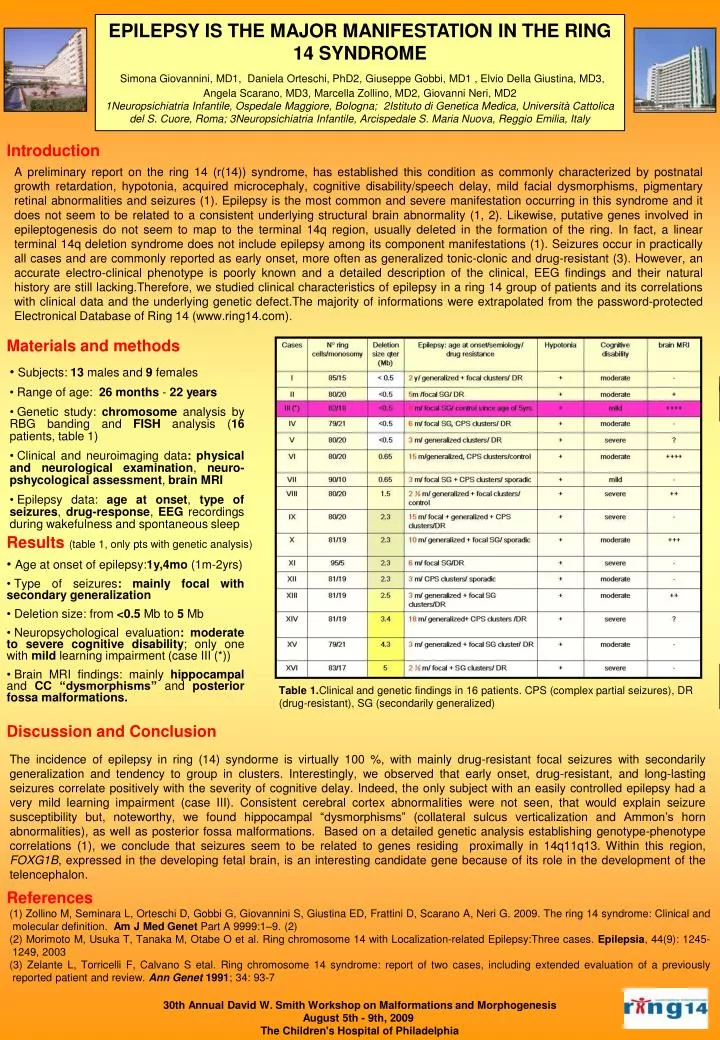
EPILEPSY IS THE MAJOR MANIFESTATION IN THE RING 14 SYNDROME Simona Giovannini, MD1, Daniela Orteschi, PhD2, Giuseppe Gobbi, MD1 , Elvio Della Giustina, MD3, Angela Scarano, MD3, Marcella Zollino, MD2, Giovanni Neri, MD2 1Neuropsichiatria Infantile, Ospedale Maggiore, Bologna; 2Istituto di Genetica Medica, Università Cattolica del S. Cuore, Roma; 3Neuropsichiatria Infantile, Arcispedale S. Maria Nuova, Reggio Emilia, Italy Introduction A preliminary report on the ring 14 (r(14)) syndrome, has established this condition as commonly characterized by postnatal growth retardation, hypotonia, acquired microcephaly, cognitive disability/speech delay, mild facial dysmorphisms, pigmentary retinal abnormalities and seizures (1). Epilepsy is the most common and severe manifestation occurring in this syndrome and it does not seem to be related to a consistent underlying structural brain abnormality (1, 2). Likewise, putative genes involved in epileptogenesis do not seem to map to the terminal 14q region, usually deleted in the formation of the ring. In fact, a linear terminal 14q deletion syndrome does not include epilepsy among its component manifestations (1). Seizures occur in practically all cases and are commonly reported as early onset, more often as generalized tonic-clonic and drug-resistant (3). However, an accurate electro-clinical phenotype is poorly known and a detailed description of the clinical, EEG findings and their natural history are still lacking.Therefore, we studied clinical characteristics of epilepsy in a ring 14 group of patients and its correlations with clinical data and the underlying genetic defect.The majority of informations were extrapolated from the password-protected Electronical Database of Ring 14 (www.ring14.com). Materials and methods • Subjects: 13 males and 9 females • Range of age: 26months - 22years • Genetic study: chromosome analysis by RBG banding and FISH analysis (16 patients, table 1) • Clinical and neuroimaging data:physical and neurological examination, neuro-pshycological assessment, brain MRI • Epilepsy data: age at onset, type of seizures, drug-response, EEG recordings during wakefulness and spontaneous sleep Results(table 1, only pts with genetic analysis) • Age at onset of epilepsy:1y,4mo (1m-2yrs) • Type of seizures: mainly focal with secondary generalization • Deletion size: from <0.5 Mb to 5 Mb • Neuropsychological evaluation: moderate to severe cognitive disability; only one with mild learning impairment (case III (*)) • Brain MRI findings: mainly hippocampal and CC “dysmorphisms” and posterior fossa malformations. Table1.Clinical and genetic findings in 16 patients. CPS (complex partial seizures), DR (drug-resistant), SG (secondarily generalized) Discussion and Conclusion The incidence of epilepsy in ring (14) syndorme is virtually 100 %, with mainly drug-resistant focal seizures with secondarily generalization and tendency to group in clusters. Interestingly, we observed that early onset, drug-resistant, and long-lasting seizures correlate positively with the severity of cognitive delay. Indeed, the only subject with an easily controlled epilepsy had a very mild learning impairment (case III). Consistent cerebral cortex abnormalities were not seen, that would explain seizure susceptibility but, noteworthy, we found hippocampal “dysmorphisms” (collateral sulcus verticalization and Ammon’s horn abnormalities), as well as posterior fossa malformations. Based on a detailed genetic analysis establishing genotype-phenotype correlations (1), we conclude that seizures seem to be related to genes residing proximally in 14q11q13. Within this region, FOXG1B, expressed in the developing fetal brain, is an interesting candidate gene because of its role in the development of the telencephalon. References (1) Zollino M, Seminara L, Orteschi D, Gobbi G, Giovannini S, Giustina ED, Frattini D, Scarano A, Neri G. 2009. The ring 14 syndrome: Clinical and molecular definition. Am J Med Genet Part A 9999:1–9. (2) (2) Morimoto M, Usuka T, Tanaka M, Otabe O et al. Ring chromosome 14 with Localization-related Epilepsy:Three cases. Epilepsia, 44(9): 1245-1249, 2003 (3) Zelante L, Torricelli F, Calvano S etal. Ring chromosome 14 syndrome: report of two cases, including extended evaluation of a previously reported patient and review. Ann Genet 1991; 34: 93-7 30th Annual David W. Smith Workshop on Malformations and Morphogenesis August 5th - 9th, 2009 The Children's Hospital of Philadelphia